

Using data to improve UK neonatal care: past, present and future
The article summarises the progress of the neonatal data landscape in the UK over the last 25 years, with particular reference to progress and achievements over the last decade. We have outlined the four main challenges faced by the current neonatal data landscape in the UK, including the need for single entry of correct and relevant data that flow to one national neonatal database; interoperability between electronic patient record systems; consistencies in quality measures; improved access to data for relevant persons and/or bodies. We have also provided our vision for the future, calling for closer collaborative working and training resources to raise awareness of the UK neonatal data landscape.
Tng Chang Kwok
Neonatal Grid Trainee and Research Fellow, University of Nottingham
Cheryl Battersby
Neonatal Consultant and Clinical Senior Lecturer in Neonatal Medicine, Imperial College London
c.battersby@imperial.ac.uk
On behalf of the British Association of Perinatal Medicine Data and Informatics Steering Group
Kwok T.C., Battersby C. Using data to improve UK neonatal care: past, present and future Infant 2023; 19(2): 54-59.
The BAPM Data and Informatics Group
The British Association of Perinatal Medicine (BAPM) Data and Informatics Steering Group welcomes the Royal College of Paediatrics and Child Health (RCPCH) strategy, which includes ‘Harnessing knowledge, data and intelligence to improve the quality of care for children and young people’ specifically ‘Using data to identify gaps and explore deficiencies in child health and services’.1
The neonatal community has long recognised the importance of data including the concept of reducing data burden for clinicians by capturing data once for a variety of purposes. Often referred to as an exemplar for other specialties the neonatal community has, over the past decade, achieved national data capture and an Information Standards Board approved neonatal dataset.2 These data have afforded valuable opportunities to inform improvements in neonatal care through national audit, quality improve-ment, service evaluation and research. However, there are concerns over the increasing complexity of neonatal data resulting from reporting demands from a range of organisations, conflicting quality measures and definitions, and multiplicity of electronic patient record (EPR) systems hampering interoperability.
In January 2021, BAPM convened a Data and Informatics Group to understand and address these concerns. The group comprises a small steering group with representation from multidisciplinary professionals and parents/patients, and a larger stakeholder group with representation from UK organisations and regions.3 Through a series of meetings, the group agreed that its remits are to:
- advocate for collection and use of accurate perinatal data for audit, research, service evaluation, commissioning, quality improvement and benchmarking to benefit babies and their families
- promote standardisation of quality measures and interoperability of EPR systems to avoid unnecessary duplication and burden for those inputting the data
- facilitate collaboration and closer working between stakeholders to streamline data collection and analysis for common purposes
- develop and share resources that will help support perinatal professionals to maximise the utility of data to benefit patient care.
This article aims to highlight progress and achievements over the last decade and to outline what is required to safeguard and future proof the continuation of national data-driven improvements in neonatal care.

FIGURE 1 The BAPM data group remit.
Successes in the last decade
Electronic neonatal data capture
EPRs were introduced from 2005, driven by the reorganisation of neonatal services into managed clinical networks and the need to share information for babies transferred between neonatal units. Over the next decade, a growing number of neonatal units adopted the neonatal-specific platform BadgerNet Neonatal Summary system, developed by an NHS-approved commercial company (FIGURE 2).4
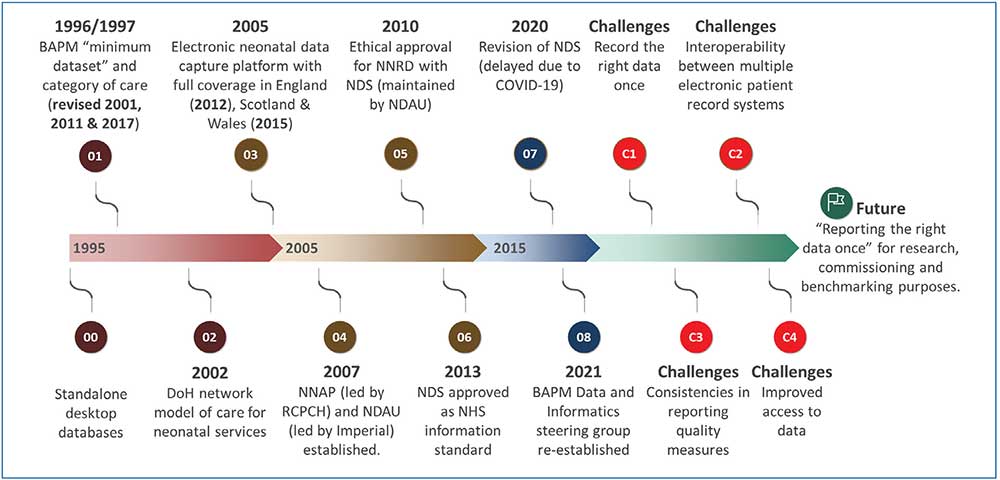
FIGURE 2 Timeline depicting the neonatal data landscape over the last 25 years and proposed future aim and challenges. Key: BAPM=British Association of Perinatal Medicine; DoH=Department of Health; NNAP=National Neonatal Audit Programme; RCPCH=Royal College of Paediatrics and Child Health; NDAU=Neonatal Data Analysis Unit; NNRD=National Neonatal Research Database; NDS=Neonatal Dataset.
Development of national neonatal datasets and a repository for national data
BAPM has long recognised the need for consistent data collection and first developed a minimum neonatal dataset in 1997, primarily to define daily levels of care. In 2007, a group of academic investigators, a network manager and a national charity representing parents established the Neonatal Data Analysis Unit (NDAU) with the aim of using standardised neonatal data for health services support, evaluation, surveillance, audit and research. In 2010, National Research Ethics approval was granted for the NDAU to curate and maintain a National Neonatal Research Database (NNRD), which would contain the national Neonatal Dataset (NDS) incorporating the Neonatal Critical Care Minimum Dataset (NCCMDS) (FIGURE 2).
The NCCMDS was developed to facilitate the National Tariff Payment System (NTPS) within neonatal critical care. It supports the NTPS by using data captured to generate a Neonatal Critical Care Healthcare Resource Group (HRG) for each calendar day of a period of neonatal critical care,5 which have been used to define neonatal activity-based income for services. BAPM developed categories of care in 1996 to enable reporting of neonatal care activity by intensive, high dependency and special care days; these were revised in 2001 and 2011,6 with an HRG update in 2016.
The NDS outlines nearly 400 data variables in the NNRD, including patient demographics, clinical interventions, diagnoses and outcomes.2 The NNRD includes data for all admissions to NHS neonatal units in England, Wales and Scotland since 2012. At present, the NNRD contains information on around one million babies and 10 million days of care, with approximately 25,000 new patients added each quarter. Researchers, clinicians, managers, commissioners, and others are able to utilise the NNRD and details of how to access it are available.7
One of the important milestones was having both the NDS (ISB 1595) and NCCMDS (SCCI0075) approved as information standards in 2013.2,5 The Data Alliance Partnership Board (DAPB) (previously the Data Coordination Board) oversees this rigorous approval process and assures the quality of information standards.8 Key advantages of having an Information Standards Board approved dataset include consistency in data variables and definitions, and facilitating the creation of a single national repository of data, such as the NNRD that can be used for multiple purposes. Importantly, the emphasis is based on the data item or variable rather than the EPR system. All EPR contractors or suppliers are expected to comply with data specifications set out in the Information Standards Notice.
The NCCMDS is currently maintained by the National Casemix Office within NHS Digital and the NDS is maintained by the NDAU, based at the Chelsea and Westminster Hospital Campus of Imperial College London.9 The NDS was last reviewed in 2022.
Measuring high quality neonatal care
“Measurement is essential for improvement” Lord Darzi.10
Interest in data has grown hugely over the last decade. The need to deliver high quality ‘value for money health care’ has necessitated the measurement, monitoring and comparison of processes and outcomes against set standards and targets. These standards are set by various organisations including the National Institute for Clinical Excellence (NICE) and government (eg the NHS Long term plan,11 Healthcare Quality Strategy for NHS Scotland12 and Quality Standards for Health and Social Care13), and are drivers for local, network and national audits and benchmarking.
The National Neonatal Audit Programme (NNAP) was established in 2006 and commissioned by the Healthcare Quality Improvement Partnership (HQIP) to assess whether babies admitted to neonatal units in England, Scotland and Wales receive consistent high quality care.14 The NNAP is funded by NHS England and the Scottish and Welsh governments and currently delivered by the RCPCH. The NNAP looks at around 10-15 areas of care provided to babies born preterm or unwell; this includes measures focussing on processes, outcomes and parental involvement in care.15 The NNAP has been an important driver for better neonatal data completeness and accuracy as well as improved quality of care.
What is needed?
Having listened to the neonatal community and a wide group of stakeholders, BAPM supports the following:
- single entry of correct and relevant data that flow to one national neonatal database
- interoperability between EPR systems
- consistencies in quality measures
- improved access to data.
Record the right data once
Over the last decade, the neonatal community has embraced and championed the ethos of ‘recording the right data once’ and using it for multiple purposes. The data needed for high quality research are the same data necessary for commissioning, audit and service evaluation. A number of other organisations have harnessed these data to drive improvements in patient care at a population level (TABLE 1). Recording data once avoids unnecessary burden on busy clinical teams and reduces errors and inconsistencies resulting from multiple entry. Lack of interoperability between EPR systems threatens the paradigm the neonatal community has successfully fostered.
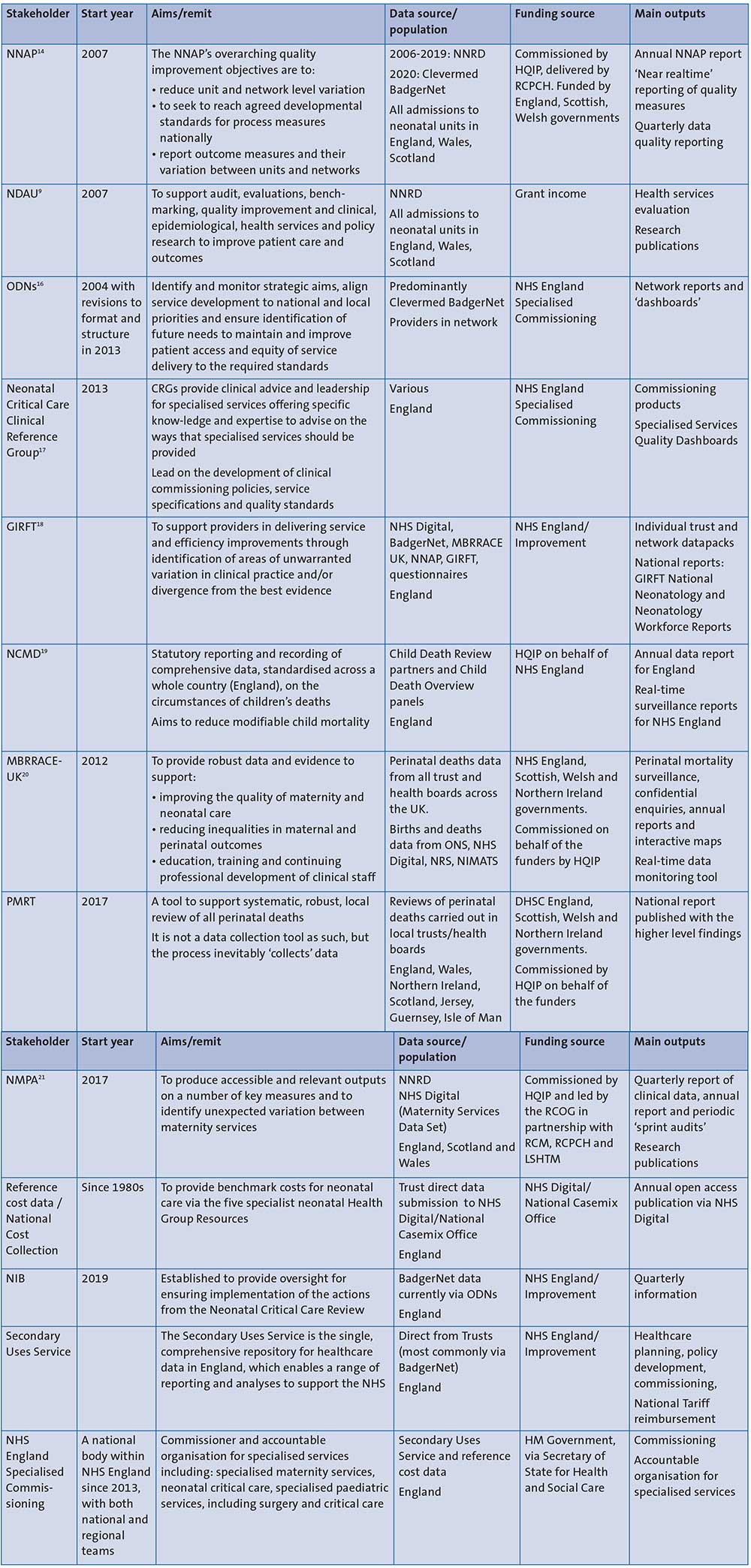
TABLE 1 Stakeholders. Key: NNRD=National Neonatal Research Database; ODN=operational delivery network; HQIP=Healthcare Quality Improvement Partnership; RCPCH=Royal College of Paediatrics and Child Health; NDAU=Neonatal Data Analysis Unit; CRG=Clinical Reference Group; GIRFT=Getting It Right First Time; MBRRACE-UK=Mother and babies - reducing risk through audits and confidential enquiries across the UK; NCMD=National Child Mortality Database; ONS=Office for National Statistics; NRS=National Records of Scotland; NIMATS=Northern Ireland Maternity System; PMRT=Perinatal Mortality Review Tool; DHSC=Department of Health and Social Care; NMPA=National Maternity and Perinatal Audit; RCOG=Royal College of Obstetricians and Gynaecologists; RCM=Royal College of Midwives; LSHTM=London School of Hygiene and Tropical Medicine; NIB=Neonatal Implementation Board.
Interoperability between multiple EPR systems
Over the last decade, having a common national electronic neonatal platform supported by a single commercial supplier has facilitated the ease of data transfer between hospitals to benefit patient care. Over the last few years, a growing number of different hospital wide EPR systems have been implemented around the country. While we recognise the financial and technical complexities of commissioning EPRs, it is essential that EPRs are able to ‘speak to each other’. Specifically, lack of interoperability between EPR systems must not result in multiple EPR systems running in parallel, eg to permit sharing data between hospitals. The latter is of paramount importance since UK neonatal care is delivered in a network model and commonly involves transfer of babies between different neonatal units. The risk of trust-wide digital solutions that are not appropriate for neonatal care or unable to support national neonatal data reporting must be considered if/when changes to EPR systems are contemplated and with this in mind, the BAPM Data and Informatics Group has convened a smaller working group to develop a service specification for neonatal data requirements. Chaired by Dr Giles Kendall, the working group aims to develop a service specification toolkit by autumn 2023 to support conversations between neonatal clinical and hospital procurement teams who are in the process of EPR procurement (further information can be found at www.bapm.org/pages/data).
Consistencies in reporting quality measures
Neonatal units share data with a number of stakeholders for benchmarking, audit, research and commissioning at local, national and international levels (TABLE 1). Understandably, each stakeholder has a slightly different focus and there is growing concern that this may lead to inconsistency in reporting measures and create unnecessary additional burden on neonatal teams inputting data. TABLE 2 contains examples of different reporting definitions for similar measures. The Neonatal Critical Care Review call for a review of capacity across neonatal services as well as improvements in standards will require consistent national as well as local data to ensure appropriate comparison(s).
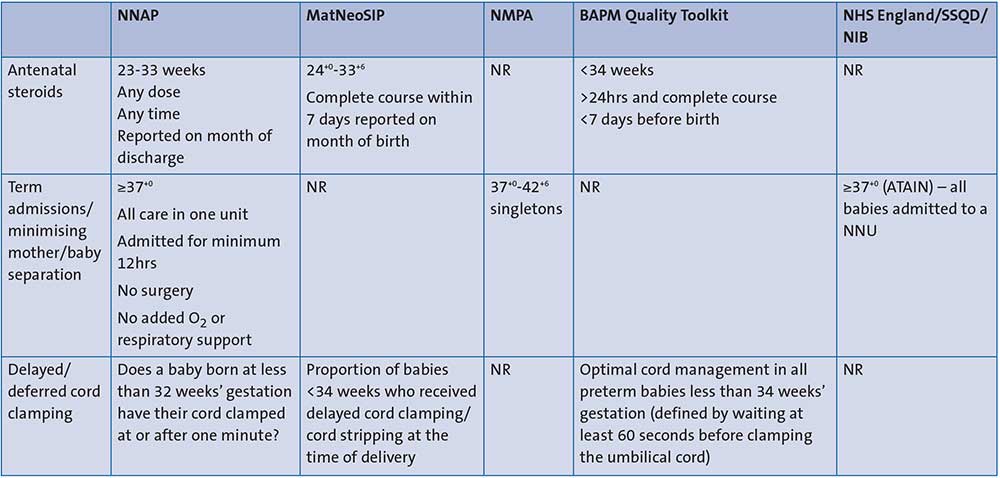
TABLE 2 Inconsistencies: examples of different definitions for similar reporting measures. Key: NR=not reported; MatNeoSIP=Maternity and Neonatal Safety Improvement Programme; SSQD=Specialised Services Quality Dashboard; ATAIN= Avoiding Term Admissions into Neonatal units programme.
The number of potential quality measures for neonatal care is vast and clinical input is required to ensure that the measures chosen have clinician buy-in. Achieving consensus in relation to definitions and measures is difficult and requires leadership from knowledgeable, professional organisations, including BAPM and RCPCH.
Improved access to data at local, network and national levels
Alongside these quality measures, demographic and activity data are also essential. Neonatal networks have a mandate to develop and implement programmes of work to improve access to specialist resources and to improve neonatal outcomes and patient experience, working closely with both providers and commissioners. Good quality data are also required for research to inform future practice. Within the necessary constraints of patient confidentiality and data ownership, we need to work together to ensure that relevant neonatal data are easily accessible to appropriate persons/organisations and used for multiple purposes.
Close collaborative working
We believe that the above needs can be met with closer collaborative working between stakeholders, hospital trusts, the neonatal community, neonatal networks, commissioning teams and commercial EPR suppliers. For example, we need to work together to find a national solution that enables different EPR systems to communicate effectively with each other. A potential solution is a national data warehouse that captures all required datasets from EPR systems in a standards compliant fashion. Such a database should allow EPR systems to pull data and act as a ‘single patient record’ for clinically critical data, thus permitting reporting at trust, network and national level to support both service design and quality improvement.
Future opportunities
Going forward, the neonatal community must continue to harness the power of population-scale data to improve neonatal care. There should be nationally agreed plans to develop data interrogation tools to facilitate more inclusive use of national data including other childhood health, education and maternity datasets to be able to interrogate outcomes over the life course. With a much more data-aware generation of perinatal professionals, BAPM strongly supports the promotion of an even deeper understanding of the importance of neonatal data and the potential to inform improvements in neonatal care. With a commitment to the development and delivery of national training resources, this article is the first step in raising awareness of the current neonatal data landscape. An electronic version of neonatal data frequently asked questions can be accessed on the BAPM website at www.bapm.org/pages/data-faqs.
Acknowledgement
The BAPM Data and Informatics Steering Group members are: Dr Cheryl Battersby (Chair), Charlotte Bradford, Dr Sanjeev Deshpande, Dr T’ng Chang Kwok, Juliette Lee, Dr Helen Mactier (2019-2022), Dr Sajit Nedungadi, Dr Stephen Wardle (BAPM Honorary Secretary, Chair BAPM Data Stakeholder Meeting), Louise Weaver-Lowe, Kirstin Webster.
The authors would also like to thank all the stakeholders within the BAPM Data and Informatics Stakeholder Group for their contribution and input to this article, especially in Table 1: Dr Eleri Adams (Getting It Right First Time), Sally Cavendish (NHS England Specialised Commissioning), Dr Ngozi Edi-Osagie (Neonatal Critical Care Clinical Reference Group), Daniel Eve (NHS England), Professor Jenny Kurinczuk (Mother and Babies - Reducing risk through audits and confidential enquiries across the UK), Professor Karen Luyt (National Child Mortality Database), Dr David Millar (Representative for Northern Ireland), Professor Neena Modi (National Neonatal Research Database), Professor Sam Oddie (Royal College of Paediatrics and Child Health), Dr Colin Peters (Representative for Scotland), Dr Oliver Rackham (Representative for Wales), Kirstin Webster (National Maternity Audit Programme) and Rachel Winch (National Neonatal Audit Programme).
Or read this article in our
Tablet/iPad edition
- The UK neonatal data landscape is an exemplar for other specialties with both a national data capture and an Information Standards Board approved neonatal dataset.
- The BAPM Data and Informatics Group identified four main challenges to overcome to safeguard current and future advancements.
- Closer collaborative working and resources to facilitate increased awareness of the current neonatal data landscape are needed to be able to properly harness the power of population-scale data to improve neonatal care.
Also published in Infant:
