

Oesophageal perforation masquerading as oesophageal atresia and tracheoesophageal fistula in a very preterm infant
This article reports a case of a preterm baby born at 28+6 weeks’ gestation with moderate to severe respiratory distress syndrome who, on initial chest radiograph, had evidence to suggest a diagnosis of oesophageal atresia and a distal tracheoesophageal fistula. He subsequently underwent a thoracotomy where this diagnosis was refuted and instead, the diagnosis of oesophageal perforation was made. We review the subtle clues that may have indicated oesophageal perforation and prevented the transfer to the surgical centre and subsequent thoracotomy.
Madhusudan Guin
Neonatal Registrar, William Harvey Hospital, Ashford, Kent
m.guin@nhs.net
Iain Yardley
Consultant Paediatric and Neonatal Surgeon, Guy's and St Thomas' NHS Foundation Trust, London
Vimal Vasu
Consultant Neonatologist, William Harvey Hospital, Ashford, Kent
Guin M., Yardley I., Vasu V. Oesophageal perforation masquerading as oesophageal atresia and tracheoesophageal fistula in a very preterm infant. Infant 2023; 19(2): 51-53.
The case
A male preterm infant was born by emergency caesarean section under general anaesthesia at 28+6 weeks’ gestation, weighing 1,350g (50th centile). The indication for emergency c-section was fetal distress. The mother had a history of preterm prelabour rupture of membranes (PPROM) at 25 weeks’ gestation and she had received a complete course of antenatal steroids. Though, there was no history of polyhydramnios on antenatal scans at 22 weeks of gestational age, the amniotic fluid index (AFI) was on the 95th centile with PPROM occurring after this.
At birth, the baby was noted to be apnoeic, blue and floppy with a heart rate of less than 100 beats per minute. He was initially managed with mask inflation, ventilation breaths (maximum inflating pressure of 20/5 and maximum fraction of inspired oxygen, FiO2, of 0.4) and was intubated in view of ongoing apnoea, likely related to maternal general anaesthesia. The initial two attempts at intubation were thought to have been oesophageal. He was intubated successfully on the third attempt with a size 2.5 oral endotracheal tube (ETT). Some blood-stained secretions were noted at the time of intubation. His airway anatomy was thought to be normal. He was mechanically ventilated and transferred to the neonatal intensive care unit. An orogastric tube was sited without resistance or complication as part of routine preterm care.
His early clinical course was characterised by clinical evidence of preterm surfactant deficiency, requiring mechanical ventilation with modest pressures (24cmH2O), FiO2 of 0.5 and surfactant therapy. A chest radiograph taken at three hours of age indicated radiological evidence of respiratory distress syndrome (RDS) and an orogastric tube coiled in the midline at the level of thoracic vertebra 2 (FIGURE 1). A clinical diagnosis of presumed oesophageal atresia and distal tracheoesophageal fistula (TOF) was made, and the baby was transferred for an urgent surgical assessment.
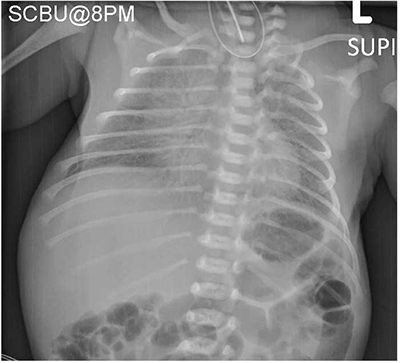
FIGURE 1 A chest and abdominal X-ray showing moderate to severe RDS and the feeding tube curled up in the throat.
Mechanical ventilation in the context of a possible distal TOF increased the urgency of referral due to the risk of preferentially ventilating the stomach over the lungs.
A Replogle tube was sited in view of the presumed diagnosis without resistance to 10cm. It was placed on low pressure suction with regular saline flushes to control saliva secretion and prevent aspiration. A repeat chest radiograph with the Replogle tube in situ is shown in FIGURE 2. Prior to transfer the infant became more unwell with evidence of persistent pulmonary hypertension of the newborn (PPHN) and required treatment with inhaled nitric oxide and systemic blood pressure support.

FIGURE 2 A chest X-ray showing the Replogle tube and feeding tube at T4-T5 thoracic vertebra. The endotracheal tube is visible at the T2 vertebra.
At the surgical centre, the Replogle tube was re-passed and found in a similar position. A right thoracotomy was performed at around 18 hours of age. The oesophagus was noted to be in continuity with the stomach and the tip of the Replogle tube was seen free in the mediastinum. A perforation of the oesophagus was not visualised but presumed to be in the neck (likely pharynx) as the Replogle tube entered the upper thorax adjacent to the oesophagus.
The Replogle was withdrawn and a 6F nasogastric tube passed to the stomach. The perforation was managed conservatively. A left intercostal chest drain was left in situ. The baby’s postoperative course was unremarkable and enteral feeds were initiated via the nasogastric tube after two days. However, his blood cultures grew E. coli and he was treated with antibiotics. He was transferred back to his local hospital five days after surgery. An oesophageal contrast study was not performed due to the site of the perforation and the need for ongoing endotracheal intubation and mechanical ventilation.
The baby was discharged from hospital at a corrected gestational age of 40 weeks and weight of 3,175g (25th centile). At the time of discharge, he was breathing air and on demand bottle feeds of maternal expressed breast milk. His developmental follow-up assessment at 16 months corrected age was appropriate.
Discussion
In this article we describe an unusual case of a very preterm infant with moderate to severe RDS, who on initial chest radiograph had evidence to suggest a diagnosis of oesophageal atresia and a distal TOF.
He subsequently underwent a thoracotomy where this diagnosis was refuted and instead, the diagnosis of oesophageal perforation was made. Although oesophageal perforation is rare and under reported, it is a known entity in preterm infants. However, we report this case because in the majority of instances, it presents later on in the neonatal clinical course and may be detected incidentally on routine chest radiography where a nasogastric tube is identified as being malpositioned.1
Extremely preterm infants are at higher risk for oesophageal perforation, which has a mortality rate ranging from 21-30% (although many of these deaths may also be attributable to comorbidities of prematurity).2 The anomalous feeding tube position may lead to complications including pneumothorax, pneumo-mediastinum and mediastinitis.
Oesophageal perforation is usually iatrogenic in nature, though it may be spontaneous. Common antecedent risk factors are procedures related to preterm neonatal care, including insertion of orogastric or nasogastric tube, tracheal suction and tracheal intubation.3 The usual site of injury to the oesophagus is at the pharyngo-oesophageal junction where the cricopharyngeal muscle works as a sling constricting the lumen. Cricopharyngeal spasm induced by insertion of a suction catheter or irritation during intubation further predisposes to injury. In addition, airway manipulation and neck hyper-extension often necessary during intubation, may also cause traumatic oesophageal injury as the oesophagus is compressed against the cervical vertebrae, obstructing the lumen.4
The rarity of the diagnosis of oesophageal perforation along with clinical and radiographic findings consistent with the diagnosis of a congenital anomaly of the oesophagus with a presentation shortly after birth, means that oesophageal perforation may not be an early medical or surgical diagnostic consideration.5 However, in this case there may have been some clues that might have alerted the clinical teams to pursue oesophageal perforation as an alternative diagnosis.
Firstly, there was no robust antenatal history of significant polyhydramnios. Although not a universal finding in oesophageal atresia, it is commonly noted. In this case, the AFI was on the 95th centile at 22 weeks, but subsequent PPROM confounded any diagnosis of developing polyhydramnios. Secondly, at delivery there was no significant difficulty noted in the baby managing his own secretions. Babies born with oesophageal atresia are commonly described as ‘frothy’ or ‘mucousy’. However, some oral secretions were noted in this case, but this may have been within the range of normality for a preterm baby following delivery. On the chest X-rays, it is apparent that the Replogle tube passes a little further than the position of the initially inserted and coiled nasogastric tube. This may have been a subtle clue indicating either oesophageal perforation or perforation of the upper pouch in oesophageal atresia. Contrast studies are not usually recommended in the diagnosis of oesophageal atresia, as the coiled radio-opaque tube is generally considered patho-gnomonic. In this case, a contrast study via the Replogle tube may have enabled conservative management6 and prevented the need for transfer to a surgical centre and subsequent thoracotomy.
Parental consent
The authors obtained written consent from the child’s parents for publication of the case history and images.
Or read this article in our
Tablet/iPad edition
- Failure to pass an orogastric tube may not necessarily indicate oesophageal atresia.
- Oesophageal perforation should be considered where repeated intubation attempts are followed by difficulty in passing a nasogastric tube.
- High index of suspicion and a preoperative contrast study or intraoperative bronchoscopy would have avoided thoracotomy.
