

Compassionate mind training: feasibility and acceptability of a staff workshop
The drive for a more compassionate healthcare system has never been more prominent. However, this has come at a time where resources across the health service are often very stretched. This article describes the feasibility of a pilot project to offer an introductory session of compassionate mind training for neonatal staff across the East Midlands Neonatal Operational Delivery Network. Feedback from the workshop demonstrates that it was very well received and that staff attending the workshop felt that further training would be useful in their roles. Future modifications and ideas for upcoming workshops are outlined.
Anita D’Urso
Consultant Clinical Psychologist
anitadurso@nhs.net
Judith Foxon
Deputy Lead Nurse, Lead for Education and Workforce
Cara Hobby
Deputy Lead Nurse, Lead for Patient and Public Involvement and Family-Integrated Care
Wendy Copson
Deputy Lead Nurse, Lead for Quality Improvement
Linda Hunn
Lead Nurse and Network Director
East Midlands Neonatal Operational Delivery Network, hosted by Northampton General Hospital
D’Urso A., Foxon J., Hobby C., Copson W., Hunn L. Compassionate mind training: feasibility and acceptability of a staff workshop. Infant 2023; 19(2): 48-50.
Compassion – feeling for a person who is suffering and being motivated to act to help them1 – is believed to have numer-ous benefits within health care, including improving clinical outcomes and increasing patient satisfaction with services.2-4 However, it is important to recognise that time must be carved out for this to be part of ongoing staff training, particularly as acute healthcare providers are required to deliver care and compassion in a high-threat, fast-paced environment.5,6 Indeed, recent systematic reviews demonstrate that incorporating compassion-focused therapy (CFT) approaches could result in practising clinicians enhancing their overall levels of compassion and empathy, as perceived by the clinicians themselves, patients, and third-party observers, using a variety of measurement tools.7,8
CFT is a therapeutic approach aimed at helping individuals cultivate compassion for themselves and others.9 The approach encourages us to respond to self-criticism by employing a self-supportive inner voice as well as examining how, as the result of evolution, we have ‘tricky brains’ that often get caught up in thinking-feeling loops.10,11 Compassionate mind training (CMT) is an essential component of CFT, using imaginal and body-based practices to bring these theoretical concepts to life – enabling us to cultivate compassion.
Individuals with higher levels of self-compassion have been found to more readily accept new challenges, modify unhelpful behaviours and recognise mistakes.12 Within a maternity and neonatal context, improvements in compassionate care have been called for in a number of recent independent enquiries.13,14 The need to explore the inhibitors and facilitators to compassionate practice within a neonatal setting is also heightened by the fact that research has demonstrated high rates of moderate to severe secondary traumatic stress and burnout in neonatal staff.15
Methods
Aims and objectives
The aim of this pilot project was to explore the feasibility of offering a ‘taster’ CMT workshop for neonatal staff working across a regional neonatal network. Commitment from busy staff often hinders staff support interventions16 but it was thought that a half day workshop would enable some introduction to the concept both individually and with colleagues. This article refers to two half-day workshops offered four months apart, both delivering the same content.
Participants
The participants were healthcare professionals (n=37) working across 11 neonatal units in a regional neonatal network. All staff from across the East Midlands Neonatal Operational Delivery Network were invited to attend. The delegates did not have to pay a fee and this cost was absorbed from the overall network training and education budget. Delegates attended from every neonatal unit within the network. The attendees included neonatal nurses from across the career pathway (n=32) midwives (n=1), consultant neonatologists (n=3) and clinical psychologists (n=1). Delegates attending came from level 1, 2 and 3 neonatal units across the network.
The workshop
CFT is rooted in an evolutionary, func-tional analysis of basic social motivational systems (eg humans’ motivations to live in groups, form hierarchies and ranks, and seek social connection).10 The CFT model divides the mind into three basic systems named the ‘three-systems model’: the threat system, the drive system and the soothing system. It has been proposed that in modern life, particularly in the com-petitive culture we have created in Western society, our emotion systems are often out of balance and mainly stimulate our threat and drive systems, at the expense of our soothing system.
A provisional layout for the workshop is outlined in TABLE 1, which was adapted from the model proposed by Lucre and Taylor (2020).17 The workshop took place over four hours in a venue accessible to all staff across the network. It was led and facilitated by a consultant clinical psychologist employed by the East Midlands Neonatal Operational Delivery Network (ODN) and was co-produced and organised alongside the Lead Nursing and Education Team within the Neonatal ODN. The first group consisted of 24 staff and the second workshop consisted of 13 staff.
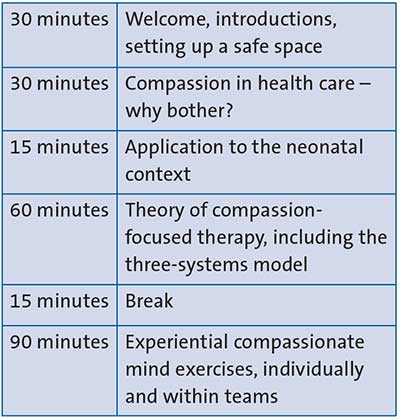
TABLE 1 The workshop programme.
The workshop was heavily interactive in nature with experiential exercises included throughout the session, in line with CMT principles FIGURE 1 demonstrates a group exercise exploring how the three-systems model applied in the group’s respective workplace environments. Within the workshop, delegates were exposed to both compassionate imagery (eg calming place imagery) and practices based on grounding (eg soothing rhythm breathing).

FIGURE 1 A group exercise to explore the three-systems model within a work context. Examples were explored about experiences that move clinicians into drive, threat and soothe modes at work.
Results
Feedback was obtained from all delegates who attended the workshops. This was collected anonymously via SmartSurvey (www.smartsurvey.co.uk) immediately following the workshop. The questionnaire consisted of a mixture of open and closed-ended questions. Overall evaluation across both workshops was positive and demonstrated that the workshops were well received. As per FIGURE 2, 97% of participants rated the workshops overall as either ‘good’ (16%) or ‘excellent’ (81%). One participant rated the workshop as ‘satisfactory’ (3%).
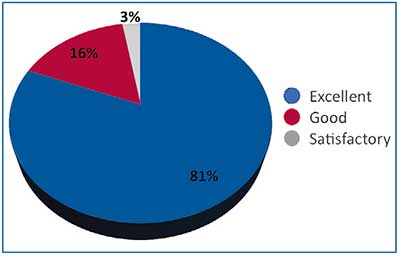
FIGURE 2 Overall rating of the workshop.
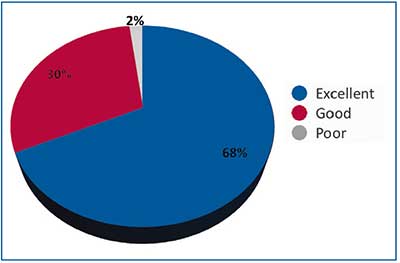
FIGURE 3 Rating of the importance of compassion in health care.
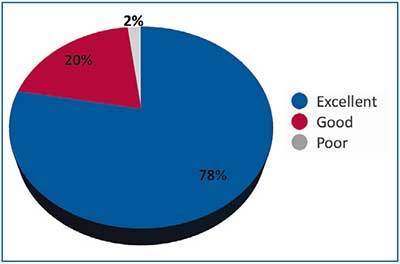
FIGURE 4 Rating of the CMT practical techniques session.
When this was explored further (FIGURES 2-4), 98% of participants rated the session examining the importance of compassion in health care as mostly good (30%) or excellent (68%). The session focused on the CMT practical techniques was rated as mostly good (20%) or excellent (78%). Analysis of the respondents’ comments identified four key themes (TABLE 2).
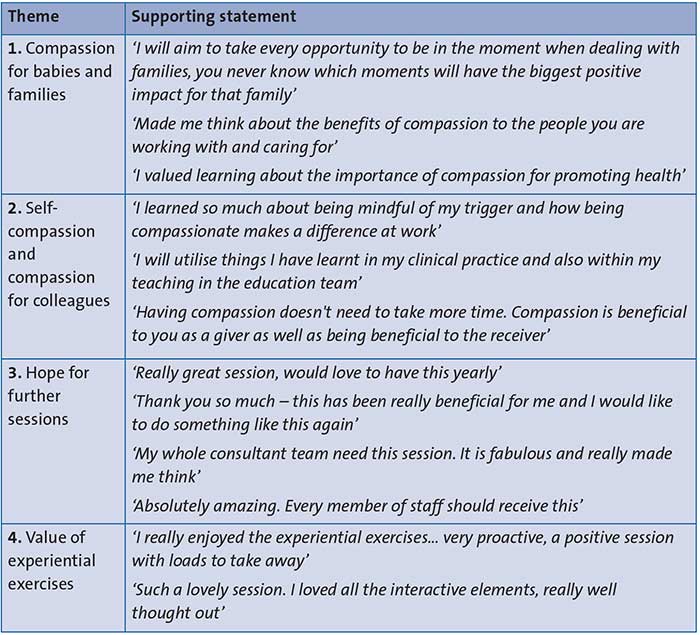
TABLE 2 Key themes and supporting statements.
Discussion
The value of CMT and compassion-focused staff support is becoming increasingly clear, particularly in healthcare settings.18,19 Indeed, a recent meta-analysis revealed moderate effect for CMT in reducing symptoms of depression, anxiety and stress, as well as increasing individuals’ levels of compassion, mindfulness and wellbeing in both clinical and non-clinical populations.20 Although previous research has reported on the benefits of CMT for student midwives,21 no previous research was identified that reported on this approach with neonatal staff. Given the elevated rates of burnout and secondary traumatic stress identified for this group of staff,15 the potential benefit of this approach appears important to explore.
Initial feedback from the four-hour CMT workshop suggests that this was very well received by staff and that it had the potential to have a positive impact on compassion for themselves, compassion towards each other and compassion towards the babies and families in their care. The interactive elements of the day were particularly valued, which is in line with the experiential style fundamental to the CMT approach. Informal feedback from delegates suggested that a half-day training session hosted within an easily accessible and central venue provided delegates with the highest possible chance of attending. From a funding perspective, the workshop was led by a consultant clinical psychologist employed by the neonatal network, thereby the sole cost incurred was for the hire of the venue, which was absorbed within the neonatal network's budget for training.
There were several limitations of the study. The number of staff who attended the workshop was relatively small (n=37), yet there was a clear theme within the qualitative feedback for further workshops to be provided for those who were not able to attend. We must consider how these approaches can become part of a wider culture change within individual units and in this regard, we have hopes that further workshops might work towards identifying ‘compassion champions’ on each unit to keep this approach alive and to help staff stay accountable for the things they aimed to work on following the workshop. We also have hopes to provide further workshops next year, as a ‘part 2’ for those who have already attended the first pilot workshops, as well as to repeat this part 1 introduction for other professionals who were unable to attend on the previously offered dates. Within this, it may be helpful to consider the use of more standardised measures of compassion (eg the Self Compassion Scale – SF22 or Compassion Satisfaction and Fatigue – ProQOL23) in order to detail any formalised shifts in compassion.
Conclusion
The pilot study detailing the results of a CMT workshop for neonatal staff demonstrated that this was very well received. Initial themes from the feedback suggest that it has the potential to have an impact on compassion for staff themselves as well as for the families in their care. Future work with larger numbers of participants and more standardised measures is warranted to explore this further.
Author contributions
AD: Led and facilitated workshop. Write up of paper. JF: Idea for the article, design and implementation. Review of draft paper. CH: Co-facilitation of the project, implementation, write up and review of draft. WC: Co-facilitation of the project, implementation, write up and review of draft. LH: Idea for the project, design, write up and review of draft.
Or read this article in our
Tablet/iPad edition
- Compassion in healthcare services is a necessity.
- A pilot project offering an introductory session of compassionate mind training for neonatal staff is described.
- Feedback demonstrates that the workshop was well received. Most staff requested further training for themselves and/or their teams.
