

Early medical closure of patent ductus arteriosus: a survey of practice in UK neonatal intensive care units
Consultant Neonatologist
Neonatal Intensive Care Unit, The Royal Oldham Hospital, Northern Care Alliance
arunoday.arunoday@nca.nhs.uk
Marianna Vidouris
Neonatology Specialty Registrar
North West Deanery, Health Education England
marianna.vidouris@nca.nhs.uk
Teck Guan Ong
Consultant Neonatologist
Neonatal Intensive Care Unit, The Royal Oldham Hospital, Northern Care Alliance
A survey was carried out to gather the opinions of currently practising consultant neonatologists in neonatal intensive care units (NICU) in the UK, regarding early medical treatment (<7 days of life) of haemodynamically significant patent ductus arteriosus (PDA) in extreme preterm ventilated babies. The survey found that consultants with cardiology and/or echocardiography interest were less inclined to agree with early medical closure than those without. It was also revealed that two thirds of the neonatal consultants surveyed performed neonatal echocardiography.
Background
The ductus arteriosus closes spontaneously in many preterm infants but prolonged ductal patency is a complication of extreme preterm birth. Longer duration of a PDA is associated with higher risk for death or bronchopulmonary dysplasia (BPD) (adjusted odds ratio=1.37; 95% CI 1.03-1.82).1
A persistently patent ductus with a large haemodynamically significant duct is associated with pulmonary hyperperfusion, systemic hypoperfusion and adverse clinical outcomes, including pulmonary haemorrhage, necrotising enterocolitis, chronic lung disease and mortality.2,3 However, to date, early medical closure has not shown significant improvement in incidence of death or moderate or severe BPD at 36 weeks corrected gestational age.4-7
There is consensus that treatment should be based on an estimate of the haemodynamic significance of the PDA. A comprehensive echocardiographic assessment, including the exclusion of ductal-dependent structural lesions, is accepted as best practice. Serial echocardiographic assessments can also guide duration of therapy and lead to a reduction in medication doses.8,9
Aims and objective
We aimed to canvas opinion regarding early medical treatment (ie pharmaceutical drug treatment to close a PDA) of haemodynamically significant PDA among consultant neonatologists in UK NICUs. We also wanted to assess any difference of opinion between those with and without cardiology and/or echocardiography interest and, for those that perform echocardiography, whether there is a unit or network guideline to follow on medical closure of a PDA.
Methodology, data analysis and results
A questionnaire was generated that surveyed the following questions:
- Are you a consultant neonatologist with cardiology interest? (Yes, no)
Do you perform neonatal echocardiography? (Yes, no)
In your opinion, would you consider early (<7 days of life) medical closure of echo-targeted haemodynamically significant PDA in extreme preterm ventilated babies (of less than 28 weeks’ gestation)? (Yes, no, not sure)
If you answered yes to question 3, does your unit or network have a guideline for medical closure of PDA that you follow? (Yes, no)
The names of all UK NICUs were compiled in a spreadsheet along with the unit contact telephone number. The neonatal secretaries for each unit were contacted and invited to share the questionnaire link with all neonatal consultants in the unit during October and November 2021. Data were collected between December 2021 and February 2022. Three reminders were sent during this period to maximise response. The answers to the survey questions can be seen in FIGURES 1-5.
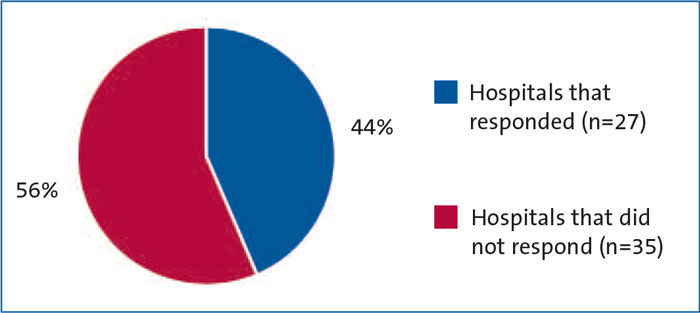
FIGURE 1 Hospital response (n=62).

FIGURE 2 Are you a consultant neonatologist with cardiology interest (n=66)?
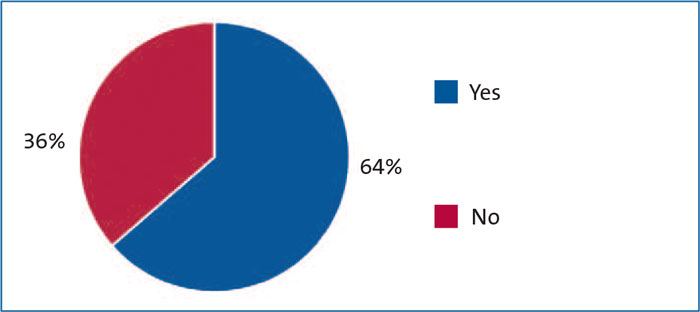
FIGURE 3 Do you perform neonatal echocardiography (n=66)?
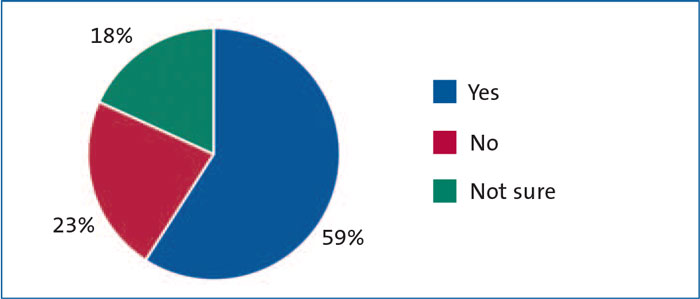
FIGURE 4 In your opinion, would you consider early (<7 days of life) medical closure of echotargeted haemodynamically significant PDA in extreme preterm ventilated babies (of less than 28 weeks’ gestation) (n=66)?
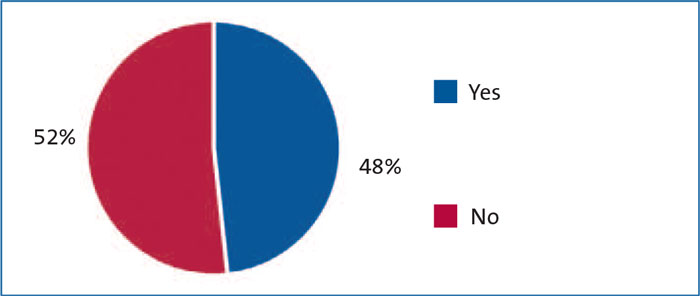
FIGURE 5 If you answered yes to question 3, does your unit or network have a guideline for medical closure of PDA that you follow (n=39)?
We analysed the data to see which consultants agreed with early (<7 days of life) medical closure of an echo-targeted haemodynamically significant PDA in extreme preterm ventilated babies (of less than 28 weeks’ gestation) – those with or without interest in cardiology and/or echocardiography (FIGURE 6). We found:
- 18 out of 36 consultants (50%) with cardiology interest would consider medical closure of PDA vs 22 out of 30 consultants (73%) with no cardiology interest.
23 out of 42 consultants (55%) with echocardiography interest would consider medical closure of PDA vs 17 out of 24 consultants (71%) with no echocardiography interest.
17 out of 34 consultants (50%) with cardiology and echocardiography interest would consider medical closure of PDA vs 16 out of 22 consultants (73%) with no cardiology and no echocardiography interest.
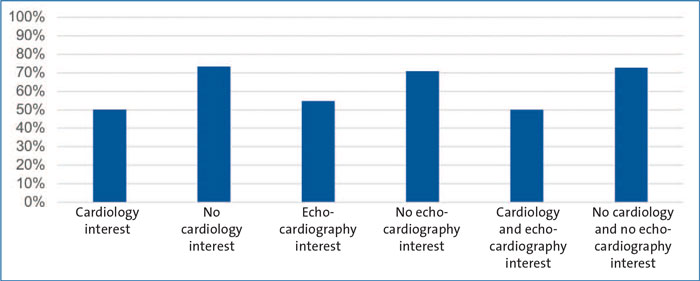
FIGURE 6 A breakdown of interest for those answering yes to question 3, ‘would you consider early (<7 days of life) medical closure of echo-targeted haemodynamically significant PDA in extreme preterm ventilated babies (of less than 28 weeks’ gestation)?
Summary of observations
- Over half of the responding neonatal consultants had an interest in cardiology.
Around two thirds of the responding neonatal consultants performed neonatal echocardiography.
Nearly 60% of responding neonatal consultants agreed with early medical PDA closure in extreme preterm ventilated babies.
Only 50% of NICUs had a unit or regional guideline for medical closure of PDA.
Consultants with cardiology and/or echocardiography interest were less likely to agree on duct closure than those without interest.
Discussion
Our survey shows that more neonatal consultants were in favour of early medical closure of a haemodynamically significant PDA, although those consultants with interest in cardiology or echocardiography tended to disagree with early medical duct closure. This might suggest that other factors, such as the duration of the PDA and exposure to PDA shunts, warrant consideration.
This survey is limited by the low number of respondents (66 neonatal consultants from 62 hospitals) and possible bias towards those with an interest in cardiology/echocardiography being more likely to respond. The survey did not allow for free text entries, nor did it consider surgical closure.
A guideline on essential echocardiographic requirements for the assessment of haemodynamic significance of a PDA is essential, especially when opting for pharmacological closure. It is concerning that many units do not have a guideline on medical closure of a PDA. Strict adherence to policy and standardisation of care, including development of a training framework and consensus between at least two senior clinicians with echocardiography skills, should be considered before medical treatment of a PDA is agreed. This would help to eliminate unnecessary exposure to cyclooxygenase (COX) inhibitors (eg indomethacin and ibuprofen) in this vulnerable population.
Acknowledgement
The idea for the article, design, implementation, conduction of the project, data analysis, and writing was performed by Arunoday. Marianna contacted the neonatal secretaries for the NICUs and distributed the survey questionnaires. Teck Guan appraised the questionnaire and assisted with its dissemination.
Or read this article in our
Tablet/iPad edition
