

The National Neonatal Audit Programme: monitoring standards of care and supporting quality improvement
Rachel Winch
NNAP Manager
Royal College of Paediatrics and Child Health
nnap@rcpch.ac.uk
Sam Oddie
NNAP Clinical Lead, Consultant Neonatologist
Bradford Teaching Hospitals NHS FT
Established in 2006, the National Neonatal Audit Programme (NNAP)1 is an ongoing audit that assesses whether babies requiring specialist neonatal care receive consistent high-quality treatment. It is commissioned by the Healthcare Quality Improvement Partnership (HQIP) and delivered by the Royal College of Paediatrics and Child Health (RCPCH).
The audit reports key outcomes of neonatal care (mortality, bronchopulmonary dysplasia, late onset bloodstream infection, necrotising entero-colitis and preterm brain injury), measures of optimal perinatal care (‘birth in the right place’, antenatal steroids, antenatal magnesium sulphate, deferred cord clamping and normal temperature on admission), maternal breast milk feeding (during admission and at discharge), parental partnership, neonatal nurse staffing levels, and other important care processes (screening for retinopathy of prematurity and follow-up at two years of age).
Key messages from the 2021 data
The summary report on 2021 data was published in November 2022.2 The report outlines the key messages and national recommendations developed by consensus by the NNAP Project Board and Methodology and Dataset Group, based on NNAP data relating broadly to babies discharged from neonatal care in England and Wales between January and December 2021. Scottish data are not included in this report; however, we hope Scottish neonatal services will re-join the audit from the 2022 data year.
Outcomes of neonatal care
The variation in rates of key outcomes of neonatal care, including mortality, broncho-pulmonary dysplasia (BPD), necrotising enterocolitis (NEC) and late onset bloodstream infection in babies born at less than 32 weeks gestational age, remains wide and concerning both across neonatal networks and between neonatal units of similar types. There is a need and opportunity to deliver significantly improved outcomes for babies if the poorest performing networks across each measure improved to the performance of the best performing. For example, rates of mortality differ two-fold between neonatal networks.
Rates of preterm brain injury (intraventricular haemorrhage, IVH, grades 3 and 4 and cystic periventricular leukomalacia) are reported for the first time this year. Missing data was a problem for 2021, but we expect data quality to improve rapidly.
The proportion of units able to provide assurance that their 2021 outcome data (NEC, bloodstream infection, preterm brain injury) are complete has fallen in the past year. High and variable rates of missing data (for example ranging from 2.6% to 55.5% across neonatal networks for IVH 3 or 4), make it difficult to interpret the results with confidence.
Optimal perinatal care
In 2021, 21.1% of babies of less than 27 weeks gestational age were not born in a maternity unit with a neonatal intensive care unit (NICU) on site. Overall, this figure is 1% worse than in 2020, following a year-on-year improvement since 2017. Evidence shows that birth in the right place reduces mortality and rates of preterm brain injury.
86.9% of mothers who delivered a baby at less than 30 weeks gestational age received antenatal magnesium sulphate. While the pace of improvement is slowing, modest further improvement with associated reduction in cerebral palsy is likely to be possible.
Just 43% of babies born at less than 32 weeks’ gestation had a minute or more of deferred cord clamping. We know that deferred cord clamping reduces mortality by 32%.3 Data from trials suggests that 60 fewer deaths may have occurred during this audit year if cord clamping had been deferred as often as it was in the trials.3 There is wide variation at both unit and network level.
73.2% of babies had a temperature measured on time and within the normal range. Between 2015 and 2021 there has been significant improvement in this measure, with a 50% reduction (26% in 2015 and 11.8% in 2021) in the number of babies who had their temperature measured on time (within one hour of birth) and who had a low temperature (hypothermic). There was no associated increase in the number of babies whose temperature was high (hyperthermic).
Parental partnership in care
Rates of breast milk feeding at discharge from neonatal care remain static (60.6% in 2021; 60.1% in 2020). Breast milk feeding rates are much higher at 14 days of age (80.5% in 2021) than at discharge, but there has been a 1.7 percentage point reduction compared to the first year of reporting in 2020. This decline may be linked to COVID-19 related impacts on unrestricted parental access to neonatal units.
There is wide variation in both breast milk feeding rates at 14 days of age and at discharge. At network level, variation in breast milk feeding at discharge is widest, ranging from 52% to 75.6%. Rates at 14 days of age range from 75.9% to 86.3%. Admission to a neonatal unit may mean that parents are unable to achieve the type of feeding they had intended. Neonatal services may also be limited in their ability to affect long-term feeding intentions, which may be influenced by socio-demographic factors.
For the first year, the NNAP reports the proportion of consultant ward rounds with at least one parent present, in addition to the proportion of admissions where a parent attended at least one consultant ward round during their baby’s stay on the neonatal unit. Data on whether parents were present were missing for 220,913 out of 808,697 (27.3%) days of admission, but where data were provided, at least one parent was present for 44.1% of consultant ward rounds.
Nurse staffing levels
Neonatal nurse staffing levels have deteriorated with 26.1% of nursing shifts not meeting recommended levels in 2021 (FIGURE 1), compared to 21.4% in 2020. In NICUs, 42.3% of shifts did not meet recommended staffing. Wide unit and network level variation exists in the achievement of recommended nurse staffing levels.
FIGURE 1 26.1% of nursing shifts did not meet recommended levels in 2021.
Care processes
In 2021, 95.4% of eligible babies received on time screening for retinopathy of prematurity (ROP) according to the NNAP definition of the screening window. This has remained between 95.1% and 95.7% over the last four years. The NNAP 2023 report on 2022 data will report adherence to the new UK screening of ROP guideline, published in March 2022.4
The proportion of babies born at less than 30 weeks’ gestation receiving two-year follow up within the appropriate time window is 72.6% (2,628 of 3,622). This is an increase since 2020, when 68.4% received a two-year follow up, and the highest proportion reported by the NNAP since the introduction of this measure in 2012. However, improvement has been slow and there is still wide variation in achievement of two-year follow up across neonatal units and networks.
Using NNAP results and resources in your service
The ‘Results at a glance’ poster (FIGURE 2) is a quick way to view national results for 12 of the NNAP metrics and signposts to more in-depth NNAP reporting and resources.
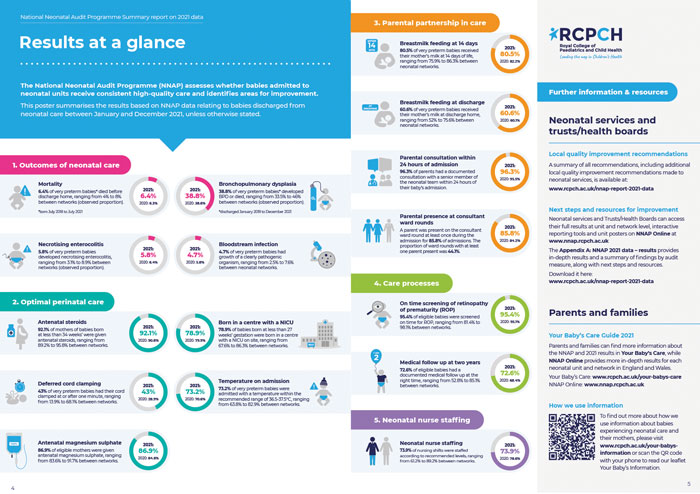
FIGURE 2 NNAP 2021 ‘Results at a glance’ poster.
National recommendations aimed at all neonatal services, networks, and national bodies are detailed by theme in the NNAP summary report on 2021 data.2 Further local quality improvement recommendations made to neonatal services are included in Appendix A, alongside more detailed results and keys findings. All recommendations, case studies and additional useful resources are additionally summarised in NNAP: Recommendations, case studies and resources on 2021 data.5
We encourage you to review the NNAP recommendations alongside your local results to formulate priorities and action plans for your service. NNAP Online6 is open-access and provides a wealth of audit data. Information at both unit and network level can be downloaded in a range of formats. Individual unit posters showing progress against 12 of the audit measures can be displayed in the neonatal unit, as well as a poster that units should adapt to indicate their action plan to address these results.
The NNAP also produces a parent guide to the annual report called Your Baby’s Care,7 which provides more detail about the 12 audit measures highlighted in the unit posters. All neonatal units in England and Wales have been sent hard copies of the unit posters for the 2021 data and Your Baby’s Care.
These documents can be very helpful to neonatal staff when talking to parents about the NNAP. In addition, NNAP Online and quarterly reports can indicate improvement opportunities.
We encourage neonatal teams to consider the best ways to share information about the audit with parents and families using their service to make sure they are aware of the NNAP, why it is important and how their baby’s information is used. You could:
- consult with your local parent group on the best way to share information
- add information and links to any online information or applications that parents in your service use
- add information about the NNAP to your unit/network parent passport
- display posters and leaflets in places where parents have time to read them such as the milk expressing room or parent lounge
- include information in neonatal admission and discharge information packs, including electronic admissions/discharge information
- consider whether sharing information about the audit ante-natally may be appropriate where there is a risk of preterm birth and neonatal admission.
QI Central is a dedicated quality improvement (QI) website that features a range of case studies focussing on audit measures. Furthermore, the British Association of Perinatal Medicine (BAPM) has QI resources including toolkits focussed on NNAP measurement areas.
What next for the NNAP?
Reviewing and validating 2022 data
Early in 2023 we will be issuing final data quality and completeness reports to units and networks giving them the opportunity to conduct a final review of their 2022 data. We will also be writing to clinical leads to ask for assurance that all of their bloodstream infection, NEC and preterm brain injury data are complete and accurate.
Updates to NNAP metrics
In 2022, we made a number of changes to the NNAP metrics to make sure they align with other national initiatives, such as the Maternity and Neonatal Safety Improvement Programme (MatNeoSIP), to enable us to report in a more timely manner by changing the cohort of interest to admitted rather than discharged babies. Key changes included:
- The antenatal steroid metric now considers whether a mother who delivers a baby between 22 and 33 weeks gestational age receives a full course of antenatal corticosteroids within one week prior to delivery.
- The ROP screening metric now aligns with the newly published RCPCH UK screening of ROP guideline.4
Full details of the 2022 NNAP metrics can be found in the NNAP 2022 measures guide.8
2023 will see some further small changes to metrics to ensure further continued alignment with other national initiatives and current guidance and guidelines. Do look out for the NNAP 2023 measures guide which will be published in early 2023.
Frequent reporting of NNAP results in the public domain
Currently the NNAP publishes annual results almost a year after the end of the data collection year. We have been commissioned to deliver more frequent reporting in the public domain from 2023, and see this as an exciting opportunity to provide more timely and high quality resources to support neonatal services to improve. Having consulted widely with our stakeholders over summer and autumn 2022, we are currently designing a reporting portal that will best suit the needs of all of our stakeholders and deliver NNAP results in the most effective way to provide quality assurance and support quality improvement.
Supporting services to reduce health inequalities in neonatal care
Throughout 2022, we have asked services to improve completeness of their postcode and ethnicity data to support reporting of NNAP metrics by ethnicity and deprivation indices. In 2023, we intend for the first time to produce supplementary national level reporting, which will enable exploration of health inequalities in the delivery and outcomes of neonatal care.
To read the most recent NNAP report:
www.rcpch.ac.uk/resources/national-neonatal-audit-programme-summary-report-2021-data
Share your QI project with a wider audience:
Email: nnap@rcpch.ac.uk
Or read this article in our
Tablet/iPad edition
