

NHS Resolution and the evolution of the Early Notification Scheme
The Early Notification Scheme was established by NHS Resolution in 2017 to commence earlier investigations into potentially severe intrapartum brain injuries with the aim of resolving obstetric claims earlier and garnering more relevant learning closer to the incident. This supports the National Maternity Ambition to halve the 2010 rates of stillbirth, maternal mortality, neonatal mortality and serious brain injuries in babies that occur during or soon after birth by 2025. This article provides a summary of NHS Resolution’s recently published second Early Notification report, The second report: The evolution of the Early Notification Scheme, and describes the changes in the scheme since its inception, highlights learning for clinical practice and makes recommendations for how NHS Resolution can further support system-level change to promote safer maternity care.
Jyoti Sidhu
Consultant Obstetrician and Gynaecologist
Barking Havering and Redbridge University Hospitals NHS Trust
Annette Anderson
Midwife and Head of Early Notification Clinical Team at NHS Resolution
annette.anderson4@nhs.net
Sangita Bodalia
Head of Early Notification Legal Team at NHS Resolution
s.bodalia@nhs.net
NHS Resolution is an arm’s length body of the Department of Health and Social Care, whose purpose is to provide expertise to the NHS to resolve concerns fairly, share learning for improvement and preserve resources for patient care. The largest area of work is handling negligence claims arising from NHS health care in England. Annually, NHS Resolution is notified of around 10,000 clinical negligence claims with an estimated value of £13.3 billion.1
The volume of claims arising from obstetric care accounts for 12% of all clinical claims by volume received in 2021-22. However, the value of obstetric claims accounts for 62% of all clinical claims incurred in the same year (FIGURE 1). The biggest contributor to high-value claims in obstetrics remains brain injuries resulting in cerebral palsy, in particular brain injuries acquired during birth.
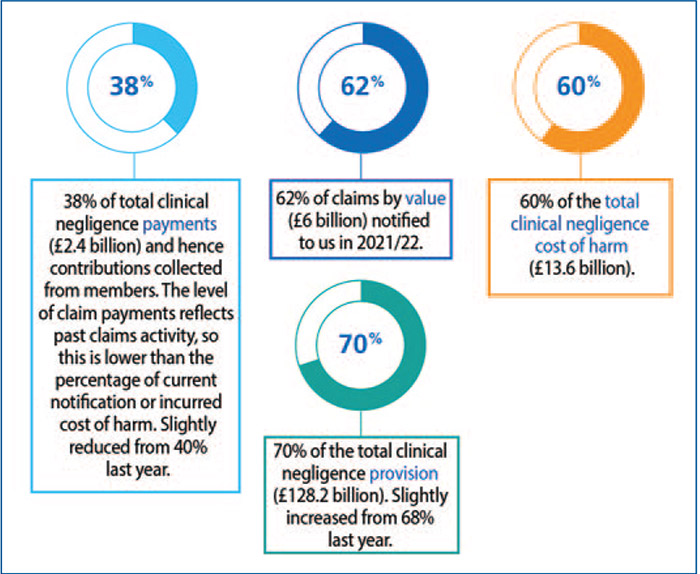
FIGURE 1 A breakdown of maternity claims in 2021/22. Source: NHS Resolution 2021/22 annual report and accounts.1
NHS Resolution’s Early Notification (EN) Scheme commenced in April 2017 with the key ambition to investigate incidents earlier, enable early admissions of liability where appropriate, and make early assessments for financial compensation. In addition, it aims to provide support to families when they need it most and share earlier learning for maternity services to improve.
In September 2022, NHS Resolution published the second report into its ground-breaking and innovative scheme that is driving proactive liability investigations and early resolution of birth injury cases to support families, staff and healthcare providers.
Although the NHS remains one of the safest healthcare systems in the world within which to give birth, avoidable errors within maternity still occur. As mentioned, maternity costs make up the largest cost to the NHS in value of claims. The EN Scheme provides a faster and more caring response to families whose babies may have suffered severe harm.
The second report: The evolution of the Early Notification Scheme provides an overview of progress made since the report into the first year of the scheme, which was published in 2019.2,3 The report updates on the progress of the key recommendations that were made in the first report and reflects on improvements to the scheme since its launch five years ago. The report also provides an analysis of the main clinical themes, based on a small cohort of cases, and makes recommendations to further improve patient safety and quality of care.
Report findings
The second EN report begins with a review of the impact of the EN scheme and progress with recommendations from the first report. These recommendations included:
- strengthening the response to harm and improving candour when an incident has occurred
- support for staff involved in maternity incidents
- a call for a standardised approach to intrapartum fetal
monitoring
- research into impacted fetal head and how to manage it
- detection of maternal deterioration in labour
- a focus on providing high-quality neonatal resuscitation.
Progress against each of the recommendations has been demonstrated. Examples include development of the Avoiding Brain Injuries in Childbirth (ABC)4 collaborative group to address issues around intrapartum fetal monitoring and impacted fetal head, and use of the Maternity Incentive Scheme5 as a lever to incentivise improving candour conversations with families and provision of high-quality neonatal resuscitation training across the perinatal team.
An analysis of 20 EN liability admissions showed the following outcomes for the babies:
- 50% had confirmed or emerging signs of cerebral palsy
- 40% of the babies sadly died within the first two years of life from injuries related to severe hypoxic brain injury
- 10% sustained a brachial plexus injury following shoulder dystocia.
All of the babies with clinical evidence of a severe hypoxic brain injury had evidence of an acute profound injury on MRI scan. The clinical themes from this cohort included delays in recognition and escalation of problems, issues with fetal heart rate monitoring and transfers of care from one location to another.
Ten EN cases involving babies with emerging or confirmed cerebral palsy within the above cohort were compared with ten traditional cerebral palsy claims (‘non-EN’ claims), which demonstrated a significant reduction of more than five years in the time from incident to liability decision, and that defence costs were two thirds less under the EN scheme than the traditional route (FIGURE 2). Small numbers notwithstanding, it is recognised that these preliminary data will form the basis of a more in-depth evaluation of the scheme, which will be explored in 2023.
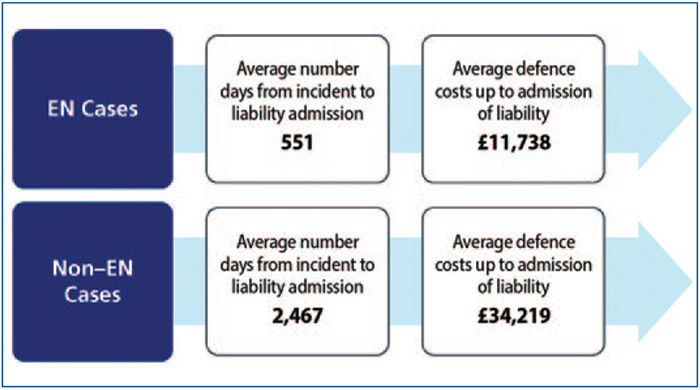
FIGURE 2 A comparison of 10 EN cases with 10 claims that followed a more traditional claims route (‘non-EN’ cases) demonstrating a time saving of approximately five years per infant/family and defence legal costs that were one third of the non-EN cohort. 1
Impacted fetal head is increasingly recognised as a significant contributor to poor neonatal outcomes. A cohort of 24 EN cases involving impacted fetal head were reviewed; although traditionally associated with full dilatation and failed instrumental delivery, 56% of these cases occurred before full dilatation. A variety of neonatal injuries were described with subdural haemorrhage being the most commonly reported injury after hypoxic ischaemic encephalopathy (HIE). There remains a shortage of information on this topic so NHS Resolution will continue to work with the national ABC programme to drive improvements in this area.
Chapter 4 of the EN report analysed a cohort of 93 cases referred into the scheme during its second year. A variety of clinical themes emerged including issues with fetal monitoring, delays in birth, evidence of infection and uterine scar rupture in women undergoing vaginal birth after caesarean section (VBAC).
Two of these themes were analysed in more detail: delayed delivery and uterine rupture in women opting for VBAC. The causes of delayed delivery were multi-factorial, involving the delivery unit’s acuity, the availability of key staff members, equipment or theatres, and the assessment of the clinical situation. The major contributors were loss of situational awareness and delay in escalation.
There was an increase in the incidence of uterine rupture in women undergoing VBAC from the first report – 42% in year two compared with 25% in year one. It is recognised that the numbers reviewed were small but key lessons remain. These include concerns about the quality of antenatal counselling and documentation of the risks and benefits associated with VBAC, administration of oxytocin and delays in recognising and acting upon uterine rupture once it has occurred.
Progress and evolution of the EN scheme
At the scheme’s inception there was no nationally agreed definition of what constituted an intrapartum severe brain injury. The Royal College of Obstetricians and Gynaecologists (RCOG) launched the Each Baby Counts programme in 20156 and created a definition to capture a broad number of babies for the purpose of learning. This definition was as follows:
All term babies (at least 37+0 completed weeks of gestation) born following labour who have a severe brain injury diagnosed in the first seven days of life, based on the following criteria;
- was diagnosed with grade III HIE, OR
- was therapeutically cooled (active cooling only), OR
- had decreased central tone AND was comatose AND had seizures of any kind.
This definition captured a large number of babies with a potentially severe brain injury, which was well-suited to the purpose of learning for future avoidance. However, for legal purposes the definition was too broad, encompassing many babies who did not have a brain injury and therefore would not be eligible for financial compensation under English law.7
A consensus opinion was formed from an expert group of obstetricians, neonatologists and neuroradiologists for the clinical definition of an EN investigation, which was agreed as follows:
Babies who have an abnormal MRI scan where there is evidence of changes in relation to intrapartum hypoxic ischaemic encephalopathy.
This definition has been used to move to an ‘outcome-first’ approach whereby cases that meet the entry Each Baby Counts criteria using the RCOG definition, are then triaged to allow investigations to be focussed on those babies most at risk of early neurological impairment and the need for early support.
The expert summit approach was developed to help streamline and expedite the legal investigative process by utilising a panel of legal and medical experts to discuss multiple cases at a single sitting. This reduction in time taken to investigate these cases means families who are entitled to compensation receive support sooner.
Additional improvements to the scheme have included the establishment of a Maternity Voices Advisory Group (MVAG)8 in January 2021 with key organisations such as the charities PEEPS-HIE (www.peeps-hie.org), Baby Lifeline (www.babylifeline.org.uk) and Action against Medical Accidents (www.avma.org.uk). The purpose of this group is to provide a forum to inform future service developments within the EN scheme and to also co-design accessible patient and family resources.
Recommendations
It is recognised that many of the clinical themes that emerged from the second EN report are not new and national workstreams are already in existence to address issues surrounding escalation, situational awareness and problems with fetal monitoring, eg the ABC programme,4 Each Baby Counts Learn and Support programme9 and ongoing QI work through the Maternity and Neonatal Safety Improvement Programme (MatNeoSIP).10
Due to the plethora of recommendations across maternity services, the second report made a limited number of new recommendations to contribute to the continued national effort to improve outcomes in maternity:
- NHS Resolution to support the work of the royal colleges and wider stakeholders to improve antenatal counselling before trial of VBAC.
- NHS Resolution to support the work of the royal colleges and wider stakeholders to improve awareness in relation to response to harm for families and staff.
- NHS Resolution to support the working relationships with NHS providers and wider stakeholders encouraging a joined-up approach between trust legal services and maternity and risk teams.
Conclusion
The second EN report demonstrates that there has been a significant reduction in the time taken to admit legal liability on cases involving a brain injury at birth. The EN Scheme has reduced the average time from seven years to approximately 18 months based on the cases analysed. This enables learning tobe identified and shared quickly, while providing early support to families when they need it most.
Some of the improvements and changes made to the scheme since its launch include focusing efforts on babies with a brain injury and where there will be the greatest impact, while streamlining investigations using innovations such as the expert summit process. The MVAG has also been set up to build closer links with families and to support the development of the scheme.
The next phase of the EN scheme will be to evaluate it from a claims, outcomes, families and staff perspective to further understand the impact of the scheme and NHS Resolution’s work.
To read The second report: The evolution of the Early Notification Scheme, visit: https://resolution.nhs.uk/wp-content/uploads/2022/09/The-second-report-The-evolution-of-the-Early-Notification-Scheme.pdf
Or read this article in our
Tablet/iPad edition
