

Introducing the new neonatal Operational Delivery Network speech and language therapists
The lack of appropriate allied health professional (AHP) expertise within neonatal care has been formally recognised in recent years. This article reviews the background to the new neonatal Operational Delivery Network AHP and psychology strategic roles and how they are working to support neonatal workforce transformation plans. We explore how an expert neonatal speech and language therapist (SLT) workforce will complement the existing medical and nursing teams’ expertise and review some of the challenges of current models of SLT provision.
Jo Marks
North West Neonatal Operational Delivery Network AHP Speech and Language Therapist
jo.marks@alderhey.nhs.uk
Zoe Gordon
Thames Valley and Wessex Neonatal Operational Delivery Network Speech and Language Therapy Lead
zoe.gordon@nhs.net
Katy Parnell
West Midlands Neonatal Operational Delivery Network Speech and Language Therapy Lead
katyparnell@nhs.net
Background
Over the past two decades there has been increasing acknowledgement that infant outcomes following admission to a neonatal unit need to extend beyond survival and discharge.1 Our expertise as SLTs in supporting early communication and feeding through skilled observation, assessment, collaborative management planning and education is well suited to the neonatal setting. Current understanding of the role of the SLT, and other AHPs, in neonatal settings remains limited and the AHP workforce is currently under-represented in neonatal care.2,3 The lack of appropriate AHP expertise within neonatal care has been formally recognised within the Neonatal Critical Care Review (NCCR, 2019)4 and neonatal Getting it Right First Time (GIRFT, 2022) reports.2,3
Murphy et al (2021)5 describe the extensive work carried out by the Royal College of Speech and Language Therapists (RCSLT) Neonatal Clinical Excellence Network (CEN) members over the past few years. The CEN is committed to developing a competent SLT neonatal workforce ensuring evidence-based intervention, providing education to achieve this, and developing outcome measures to evidence the impact of SLT interventions. SLTs work in collaboration with parents, families and with members of the neonatal team in the areas of early communication, feeding and swallowing.5 SLTs play a core role in the delivery of proactive, evidence-based neuroprotective care, which can support families and the neonatal workforce through direct interventions and education. TABLE 1 summarises the breadth of the neonatal SLT role.
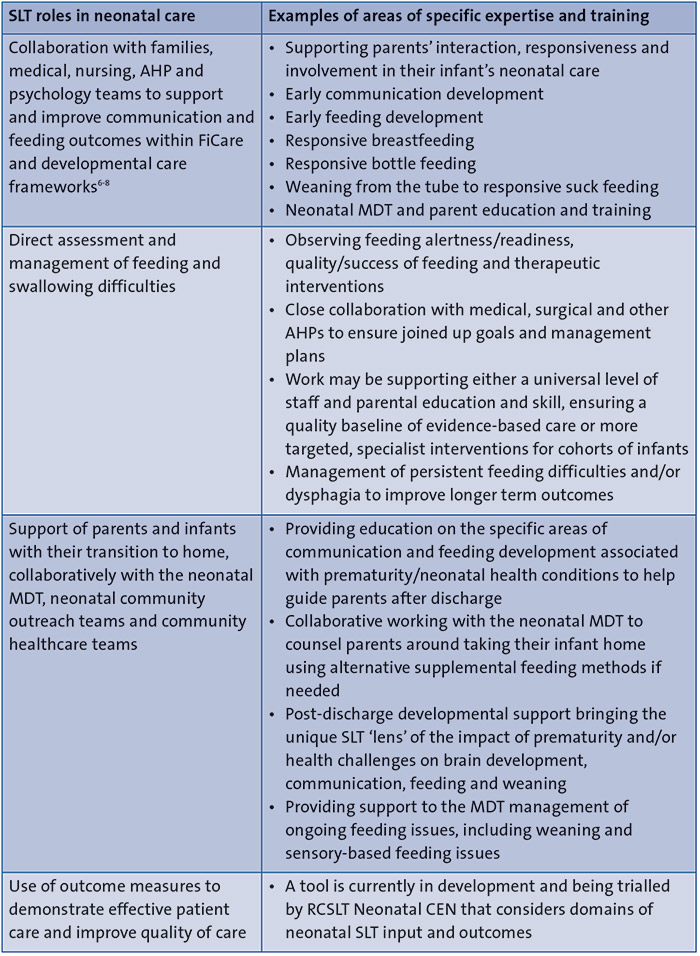
TABLE 1 Summary and examples of the range of SLT roles and skills relating to neonatal care. Key: MDT=multidisciplinary team; FiCare=family-integrated care.
National drivers for neonatal change
The Toolkit for High Quality Neonatal Services (2009)9 and the British Association of Perinatal Medicine (BAPM) Service Standards for Hospitals Providing Neonatal Care (2010)10 recognised the need for AHPs within the neonatal unit. In 2018, the RCSLT Neonatal CEN developed SLT whole time equivalent (WTE) staffing recommendations based on national benchmarking11 to clearly identify the SLT workforce short fall with an aim to consider the development of business plans to increase service provision. These staffing recommendations are supported by professional competency documents to ensure SLTs reach the required standard to practise in neonatology. Similar developments have been made by our neonatal AHP and psychology colleagues.
The NCCR4 set out to review neonatal care resulting in a specific action plan for regional commissioning teams with the neonatal ODNs to bring about a service change. These recommendations have been recently supported by the GIRFT programme (2021/2022)2,3 and the Ockenden report (2022).12
As a consequence of the NCCR recommendations, each neonatal ODN was commissioned to establish an AHP and psychology team working at a strategic level to contribute to neonatal service development and workforce transformation plans. The aim is to ensure a holistic, equitable and cohesive approach to the delivery of neonatal care for infants, families and the neonatal workforce (FIGURE 1).

FIGURE 1 The 2019 NCCR report4 recognised the valuable role that SLTs play in neonatal care.
Neonatal ODN AHP roles in England
Neonatal ODN AHP roles have been in place in the West Midlands since 2009. These AHP roles consisted of a respiratory physiotherapist, a dietitian and an SLT. The Southern West Midlands Newborn Network (SWMNN) employed ODN AHPs with the aim to fulfil the recommendations of the Neonatal Toolkit9 and the BAPM Service Standards.10 This established team has provided an example of the implementation of these new AHP and psychology roles.
Each neonatal ODN in England now has AHP and psychology teams established, consisting of dietetics, occupational therapy, physiotherapy, SLT and psychology. There are 12 SLTs in post within the ODNs across England, all of whom also continue to carry neonatal clinical specialist roles and are active members of the RCSLT Neonatal CEN. These SLTs are working alongside their neonatal ODN clinical and strategic leads, other neonatal ODN AHPs and psychologists, and local neonatal AHPs to scope and support the neonatal workforce, quality, and education workstreams, highlighting the value of increased AHP and psychology services in neonatal care.
Models of SLT service delivery to neonatal care
Access to specialist neonatal SLT is extremely variable. Access to therapists can be limited and with differing levels of experience. Where SLT provision does exist, some of these services are not clearly funded by or embedded in neonatal services resulting in inequitable service delivery within and between neonatal ODNs. ODN SLTs are currently mapping the myriad of different sources of funding, models of service provision, SLT competency and skill mix. For example, in-reach services from community providers versus funded embedded services that currently exist nationally. Early involvement of SLT embedded in the care for our neonatal infants and families enables individualised and family-centred care, supports therapeutic interventions and improves longer-term outcomes. TABLE 2 compares some of the risks versus benefits related to service delivery models.
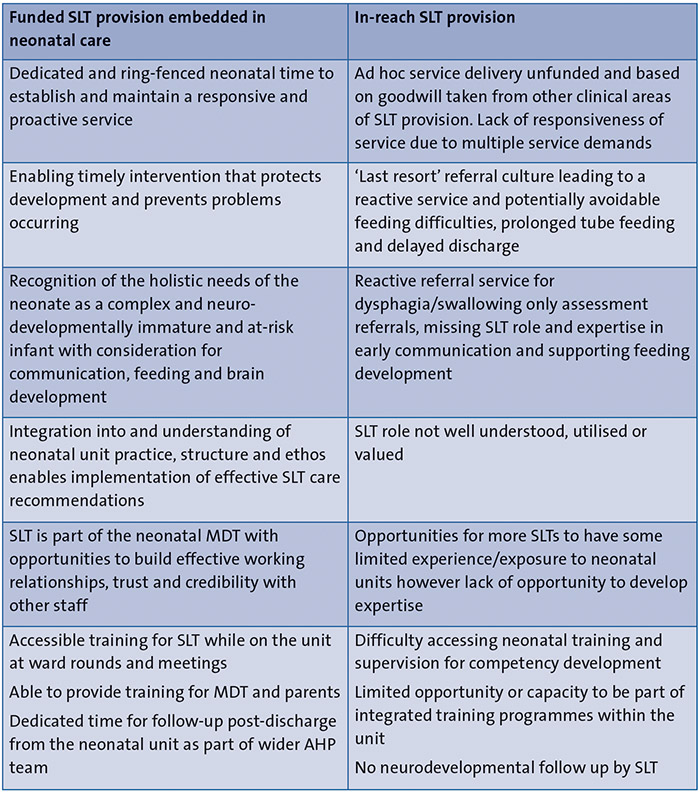
TABLE 2 The risks versus benefits of the two different service delivery models.
Conclusions
Recent reports into service provision and staffing in neonatal care have emphasised the value of AHPs and psychologists. This has led to more SLTs in neonatal care and for the first time SLTs in strategic neonatal ODN roles, enabling them to begin to highlight the SLT role, address service inequalities and consider staffing provision.
It is important that SLTs, together with neonatal medical, nursing, AHP and psychology colleagues, continue to raise their profile at a national and local strategic level to influence change and demonstrate the skills and expertise brought to the neonatal workforce and the benefits in improving infant and family outcomes throughout their neonatal care journey. Key relationships built between neonatal ODN SLTs and local SLTs within neonatal units will further support specific workstreams and service developments while continuing to develop a robust and resilient workforce for the future.
SLTs working in neonatal care can access resources from the RCSLT Neonatal CEN5 and local and national neonatal ODN teams. These include the recent Health Education for England (HEE) e-learning for healthcare (e-lfh) foundation modules, including Introduction to Allied Health Professionals in Neonatal Care and a further two profession-specific modules focused on the role of the SLT within neonatal care and development of clinical skills and knowledge.13
The AHP and psychology neonatal ODN roles are not only a resource for unit neonatal AHPs and psychologists, but are also an excellent resource for the wider neonatal MDT including medical and nursing teams. We recommend multidisciplinary engagement across neonatal teams with the neonatal ODN AHP and psychology teams. Information on local neonatal ODN AHP and psychology teams and available supporting resources are available on each neonatal ODN website.
If you are an SLT working within a neonatal unit we would encourage you to reach out and contact your ODN SLT to access support, education and share best practice within your network.
Acknowledgement
The authors’ thanks are extended to members of the RCSLT Neonatal CEN committee, in particular the Neonatal ODN SLTs.
Or read this article in our
Tablet/iPad edition
- SLTs deliver proactive, evidence-based neuroprotective care.
- Current access to specialist neonatal SLT is extremely variable.
- Where SLT provision does exist, some services are not clearly funded by or embedded in neonatal services resulting in inequitable service delivery.
- AHPs and psychology lead roles are now integrated into each neonatal ODN to support workforce and education transformation plans
Also published in Infant:
