

An evidence-based initiative to increase use of own mother’s milk in a NICU: the impact of COVID-19
This article describes a quality improvement approach to increase the use of own mother’s milk (OMM) during the first 14 days of life for infants admitted to the neonatal intensive care unit of a neonatal tertiary centre in Portugal. The project coincided with the COVID-19 pandemic, providing an opportunity to assess the impact of COVID-19 on lactation practices and OMM doses.
Catarina Garcia
Neonatologist
Tânia Marques
Neonatologist
Leonor Antunes
Nurse Specialist in Child Health
Sónia Semião
Chief of Nursing (Neonatal and Paediatric Intensive Care Unit)
Rosalina Barroso
Head of NICU
maria.r.barroso@hff.min-saude.pt
Neonatal Intensive Care Unit, Hospital Fernando Fonseca, Amadora, Portugal
Background
The benefits of breastfeeding for both infant and maternal health are well established,1 and hence World Health Organization (WHO) guidelines recommend exclusive use of human milk for all infants, particularly preterm infants.2,3 The importance of human milk, particularly OMM, is even more profound for infants in the neonatal intensive care unit (NICU). In this setting, OMM is known to be superior to both donor human milk (DHM) and formula, as it reduces rates of complications such as necrotising enterocolitis, late-onset sepsis, retinopathy of prematurity and length of stay.4
Uninterrupted availability of OMM is key to supporting exclusive OMM feeding in NICUs and a number of evidence-based lactation best practices exist to improve the availability of OMM. These include early expression (within three hours after birth),5-7 frequent expression (every 2-3 hours, aiming for eight or more in 24 hours),8-10 and effective expression (double pumping with a hospital grade electric breast pump).10-12 However, while these practices are associated with more mothers coming to volume (consistently achieving >500mL per day before day 14), and increased doses of OMM for NICU infants across their hospital stay, there is a lack of data on how well these practices are being implemented.8,10,13,14 This is a cause for concern, since there is evidence that a sub-optimal number of infants in NICUs receive human milk throughout their hospitalisation, commonly reported as due to a low milk supply.10
Aim
Quality improvement (QI) initiatives have been shown to be effective in increasing the amount of human milk and improving breastfeeding in hospitalised infants.10,15,16 This paper describes a QI approach adopted at a neonatal tertiary centre in Portugal. After assessment of the neonatal centre with the NICU scorecard,17 a QI approach was designed to improve coming to volume in mothers of all infants admitted and improve OMM feeding for very low birth weight infants (VLBW) through implementation of evidence-based lactation practices. The project coincided with the COVID-19 pandemic, providing an opportunity to assess the impact of COVID-19 on lactation practices and OMM doses.
Methods
A core research team for the project was established including neonatologists, nurses and a physiotherapist. A project timeline was drawn and outcome measures were defined. All newborn infants admitted to the NICU with a length of admission >14 days were included. Exclusion criteria were length of admission <14 days, formal contraindication for OMM and outborn infants.
QI project timeline
The QI initiative was initially divided into two phases: first assessing the baseline OMM dose in the NICU without any intervention and then evaluating the results after education, training and interventions. With the COVID-19 pandemic, the project was restructured into four phases and conducted between July 2019 and June 2021 (FIGURE 1).
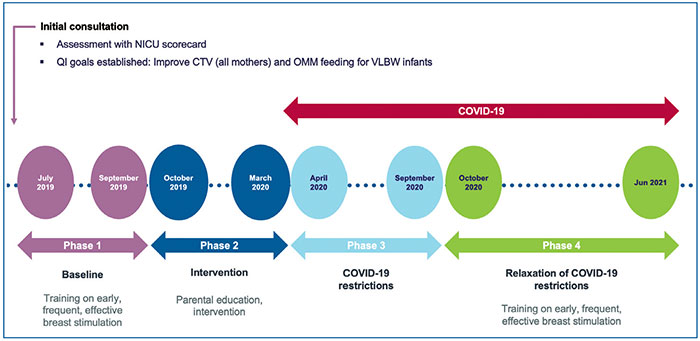
FIGURE 1 QI project timeline, July 2019 to June 2021. Key: CTV=coming to volume; OMM=own mother’s milk.
Phase 1: Baseline assessment of OMM dose
Data were extracted for each case file and for each day for the first 14 days after birth or until discharge, whichever came first. In addition, the composition of daily feeds was recorded according to feed type (OMM, DHM, or formula). These data served to demonstrate the current status of OMM dose in the NICU. While expression practices were not recorded, the data represented the outcome of these practices, and were thus a good indicator of the need for improvement.
Phase 2: Intervention – improvement and measurement of key lactation practices
A series of measures were implemented to improve expression practices and use of OMM such as:
- effective training on evidence-based lactation practices to healthcare professionals including the NICU and the maternity, labour and delivery wards
- increasing the number of pumps available and implementation of an early, frequent and effective expression protocol with double pumping use.
Two information leaflets were designed and distributed to parents: one regarding the importance of OMM and another explaining step-by-step how to use double pumping breast expression machines with a training video available through a QR code. Outcomes of this phase were assessed from expression and feeding log data from each enrolled newborn infant.
Phase 3: Implementation of COVID-19 related measures in the NICU
In April 2020, COVID-19 hit Portugal and restrictions were implemented on day-to-day hospital life. Most infants born to SARS-CoV-2 positive mothers stayed with their mothers, following rooming-in policies. When admitted to the NICU (either for maternal or newborn conditions) they stayed in a negative pressure ward. None of the babies born to SARS-CoV-2 positive mothers were admitted for more than 14 days and hence were not included in this study. Hospital measures related to prevention of transmission of COVID-19 were implemented, including:
- earlier postpartum discharge of all mothers
- fewer breast pumps to loan for home use
- restricted NICU parental visits (mothers restricted to a six-hour period per day)
- reduction of NICU cots
- increased nursing workload and separation of staff between COVID-19 infected/non-infected mothers and babies.
During phase 3, the outcome of the implementation of these COVID-19 measures was assessed.
Phase 4: Relaxation of COVID-19 restrictions in the NICU
During this period, COVID-19 restrictions were lifted (no time restrictions for mothers, fathers were allowed to visit every other day, breast pumps were available to loan for home use).
Outcome measures in the QI project
Outcome measures in this study were:
- time to first expression, defined as the time from delivery until first documented expression and categorised as within three hours, 3-6 hours, 6-12 hours and >12 hours
- frequency of expression, measured from expression logs provided to the mothers. It was defined as the frequency of any breast stimulation event (breast pump expression, a breast feed, manual expression) during a 24-hour period. Effective expression practices (eg double pumping) were also documented. Maternal daily milk volumes were recorded from the mothers’ expression logs.
- OMM dose, recorded from feeding logs.
Monthly monitoring and evaluations were conducted to ensure that the interventions were being effectively implemented and that ongoing improvements were being observed.
Data on feeding and expression events were entered into an offline data collection tool (Medela Lactation QI, Medela AG Switzerland). Multi-patient summaries were exported from the data collection tool for the respective time periods and descriptive analyses were conducted. The project was approved by the hospital’s ethical commission. Verbal consent from parents was obtained for enrolment in the project.
Results
Demographics
The Fernando Fonseca Hospital is a public neonatal tertiary referral centre covering the Lisbon metropolitan area. The population is multicultural, approximately 50% being immigrants, and a significant proportion in low socio-economic groups. The NICU is a medical surgical level III unit with 20 beds. It admits approximately 300-350 newborn infants each year, of whom 20-25% are preterm infants under 32 weeks of gestational age, under 1,500g in weight, or both.
During the project a total of 187 newborn infants were enrolled. Overall mean gestational age was 31 weeks (23-41 weeks) and mean birth weight 1,539g (590-3,305g). During the COVID-19 pandemic (phases 3 and 4), the number of NICU beds was reduced to 18. Of these, four were reserved for newborn infants born to mothers with COVID-19 (preterm or critically ill infants). TABLE 1 describes the characteristics of mothers and infants receiving care in the NICU in each phase of the project.
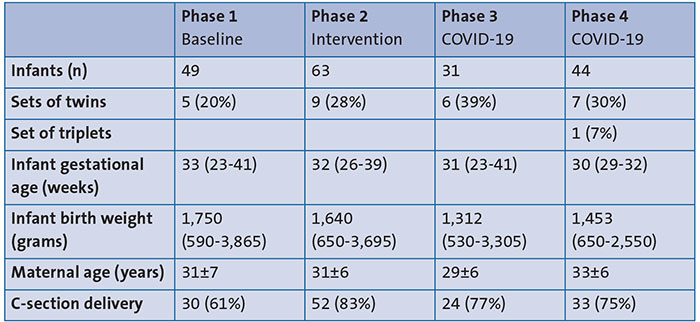
TABLE 1 Characteristics of mothers and infants receiving care in the NICU in each phase
of the project.
Phase 1: Baseline assessment of OMM dose
A total of 49 newborn infants were assessed with 25% VLBW and 12% extremely low birth weight infants (ELBW) of less than 1,000g. In this baseline data the average dose of OMM in the NICU over the first 14 days was 43%. This was particularly low in the first few days with 92% of newborn infants receiving formula on the first and second days of life.
Phases 2 to 4: Impact of interventions
In the first intervention phase a total of 63 newborn infants were assessed. In this group, 21% were VLBW and 17% ELBW. During phase 3 (COVID-19 first measures), 31 newborn infants were enrolled with a high percentage (36%) of ELBW infants, while during phase 4 (relaxation of restrictions) from a total of 33 newborn infants, 46% were VLBW and 18% ELBW.
Dose of OMM
After implementation of lactation practices in the NICU, the mean dose of OMM increased from 43% during phase 1 to 57.6% during phase 2, representing a 34% increase. In the VLBW group 76% of feeds were OMM in the first 14 days of life.
With COVID-19 restrictions (phase 3), there was a significant decrease in this parameter to 39.2%, especially in the first days when practically all infants were formula fed. When measures were lifted (phase 4) there was an improvement to rates better than in any other previous period with 72.5% of OMM and 75% OMM in the VLBW infant group.
Time to first expression
During phase 2 (intervention and implementation of lactation practices), 12% of mothers had their first expression documented to be within three hours after delivery, while 59% of mothers had their first expression documented as >12 hours after delivery (FIGURE 2).
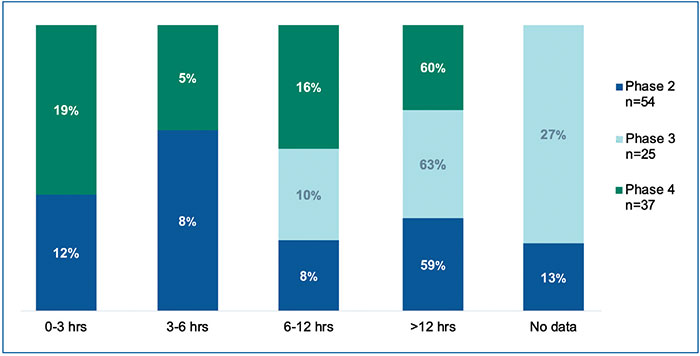
FIGURE 2 Time to first expression.
COVID-19 related changes in clinical practice in force from April 2020 were associated with a reduction in the number of mothers pumping early after delivery: no women were documented as having their first expression within six hours after delivery during the period from April to September 2020 (phase 3), and 63% did not start pumping within 12 hours after delivery (FIGURE 2). With the lifting of restrictions from October 2020 onwards there was a significant increase in mothers’ first expression in the first three hours to 19%, a higher percentage than when lactation practices were first implemented.
Frequency of expression
Between October 2019 and March 2020 (phase 2), the mean daily number of expressions increased from approximately 3.0 on day 1 after birth, to 4.5 at day 7 (FIGURE 3). The frequency of expression decreased during the period from April to September 2020 (phase 3), with mean values of 1.3 on day 1 after birth and 3.4 on day 7 (FIGURE 3). From October 2020 to June 2021 (phase 4) there was a considerable increase in the frequency of expression compared to phase 3.
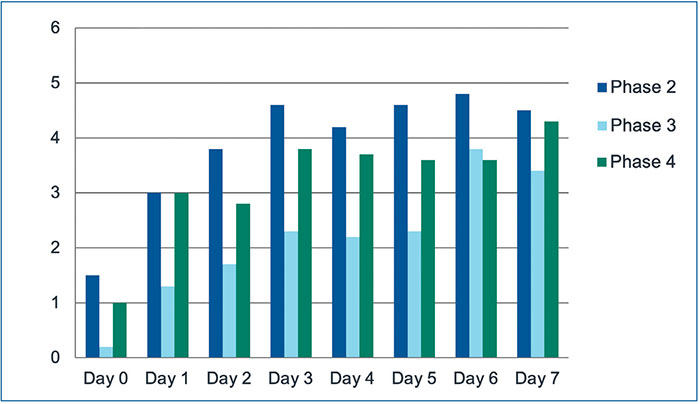
FIGURE 3 Average expression frequency.
Maternal daily milk volumes
During phase 2, the maternal daily milk volume increased progressively during the first week after delivery, with mean values of 278mL reached on day 7 (FIGURE 4). Following the implementation of COVID-19 related practices, mean daily milk volumes decreased (163mL on day 7). During phase 4 there was a boost in the mean value and the goal of achieving >500mL/day was slightly closer than during phase 2.
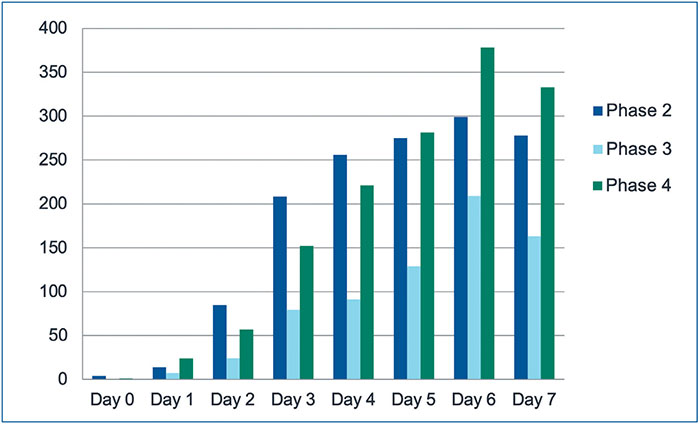
FIGURE 4 Average maternal daily milk volume (mL).
Discussion
Quality improvement of key lactation practices is an effective approach for increasing the dose of OMM for hospitalised infants, including those treated in NICUs.10,15,16 Consistent with previous studies, this study has shown that substantial improvements in the availability of OMM can be made in a short time period when evidence-based lactation practices are implemented. As described during phase 2, there was an increase in OMM during the first 14 days, especially in VLBW newborn infants.
This study, however, has also highlighted the substantial negative impact on the availability of OMM of COVID-related practices aimed at reducing infection risk. During the course of the pandemic:
- the time to first expression increased
- the frequency of expression decreased
- key markers of effective lactation (such as maternal milk volume and OMM dose) were reduced.
The likely driver for the reduced availability of OMM was the reduction in frequent and effective expression, since frequent and effective stimulation and milk removal from the breast in the early hours and days after birth are essential for mothers to effectively initiate and build milk supply.8-12,18
Key COVID-related measures, such as visiting restrictions, reduced admittance of parents to the NICU and limited access to hospital-grade double breast pump technology, also had the effect of reducing frequent and effective milk expression. In addition, national lockdown restrictions created further, indirect, barriers to effective breastfeeding and OMM use. For example, reductions in public transport services led to reliance on partners or family members for transport to hospital, particularly after caesarean deliveries, while childcare for siblings was hampered by school closures and decreased nursery facilities. The COVID-19 pandemic also significantly reduced access to hospital-grade breast pumps at home, thereby impairing the frequency and efficacy of pumping. NICUs stopped free loan of hospital-grade pumps, and many rental stations that were located in community pharmacies within retail outlets were closed during the pandemic. For these reasons, mothers were encouraged to source their own personal-use pump, but cost was often a significant limitation as breast pumps are currently not reimbursable in Portugal.
The impact of COVID-19 on breast-feeding and OMM use was exacerbated by earlier discharge for mothers. During phases 1 and 2 of this study, the mean time of maternal discharge after birth was 36 hours for normal vaginal delivery and 72 hours for caesarean sections. Following the implementation of COVID-related measures, these times decreased to 48 hours for caesarean sections.
With the relaxation of COVID-19 measures there was also an improvement in the team organisation (namely bringing to the research team two nurses from the delivery room and maternity ward team) and the certainty of the need to enhance overall lactation practices. This effort is reflected especially in the increase in time to first expression rates in the first three hours as well as in expression frequency. During phase 4 there was also an awareness of the need to improve records, since only accurate registers reflect true current NICU daily practices.
Conclusion
In conclusion, considerable improvements in the availability of OMM were made in a short time by implementing evidence-based lactation practices. However, essential COVID-related practice changes provided an unintended, yet dramatically negative, impact on lactation care and the subsequent feeding of OMM to NICU infants. Therefore, COVID measures should be carefully assessed for any resulting barriers to frequent and effective expression, in order to maintain uninterrupted availability of OMM for infants in NICUs.
Acknowledgements, funding and author contributions
In addition to the authors, there was a team responsible for the implementation of the project in the NICU, namely: Ana Paula Castro, Beatriz Fraga, Daniel Lanzas, Filipa Santos, Madalena Carvalho, Paula Costa and Teresa Aguiar. Ingrid Gouveia was part of the hospital research team. We would like to thank Medela for support during the project.
The project did not receive any funding. The personal-use breast milk collection sets were charged to hospital expenses and the hospital-grade electric breast pumps were provided by the manufacturer (Medela AG, Switzerland).
All authors contributed to the design and the development of the project. LA trained the NICU team in lactation best practices. SS coordinated the training team. TM and CG collected, registered and analysed the data. RB reviewed the final manuscript.
Or read this article in our
Tablet/iPad edition
- Quality improvement practices can increase the dose of OMM use in neonatal care units.
- Motivated and trained staff and increased availability of hospital-grade electric breast pumps can increase early, frequent and effective breast milk expression practices in the NICU.
- Measures aimed at reducing COVID-19 transmission had an unintended negative impact on OMM use in the NICU.
Also published in Infant:
