

Why do babies ‘bounce back’? A review of ScotSTAR neonatal transfers following repatriation over a four-year period
Tayyaba Yasmeen
ST6 Neonatal Grid Trainee,
tayyaba.yasmeen1@nhs.net
Allan Jackson
Consultant Neonatologist, Princess Royal Maternity Hospital Glasgow, Neonatal Lead ScotSTAR
ScotSTAR Neonatal Transport Service, Scotland
Background
The safe transfer of sick neonates is an essential component of neonatal care, enabling all babies to receive specialist care when required. Repatriation of babies and families to their local units is not only desirable but also critical, due to a high demand for cots in specialist services and neonatal intensive care units (NICUs). When an infant requires transfer back for a higher level of care following repatriation (a ‘bounce back’), concerns are often raised about repatriation pathways; however, there is a lack of data on this phenomenon.
Methods
We reviewed the data of all neonatal transfers by ScotSTAR (the Scottish Specialist Transport and Retrieval Service) where a baby had a transfer from a level 3 unit, to a lower-level unit but subsequently required transfer back to a higher level unit for uplift of care. This was a retrospective review of electronic records from February 2016 to January 2020. The following groups were selected for further analysis:
Category 1 Born in a level 3 NICU after in utero transfer, repatriated to a level 2 local neonatal unit (LNU), deteriorated/needed specialist review or investigations and returned back to the NICU.
Category 2 Born in a LNU, transferred to level 3 centre for escalation of care, repatriated but then returned to the level 3 centre for investigations or specialist review.
Category 3 Born in a level 3 centre, transferred for cardiac/surgical care to a ‘specialist centre’, repatriated back to the level 3 centre but returned to the specialist centre due to complications/further specialist review or investigations.
Other variables studied were gestational age and birth weight.
Results
There were 5,090 neonatal transfers in total carried out over the four years. Of these, 1,854 were repatriations (FIGURE 1).
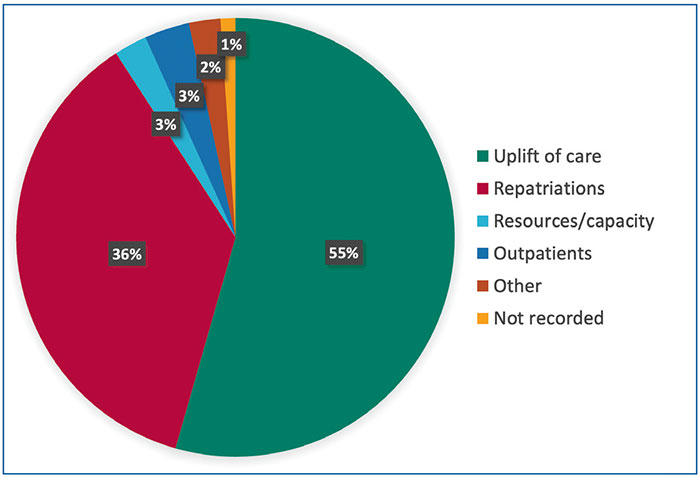
FIGURE 1 ScotSTAR neonatal transfers, February 2016 to January 2020.
Based on the inclusion criteria, there were 68 bounce back episodes (3.7% of repatriations) in 64 babies over the period of four years. The median gestational age was 28+2 weeks (range = 25-41+6 weeks’ gestation) and the median birth weight was 1,102g (range = 650-4,030 g). Of the 64 babies that bounced back:
- 61% (n=39) of neonatal transfers were classified as category 1
- 30% (n= 19) were classified as category 2
- 9% (n=6) were classified as category 3.
26% (n=18) of babies were transferred back to the level 3 unit within 72 hours of initial transfer, while 74% (n=50) were transferred back at >72hours.
57% (n=39) were elective transfers and 43% (n=29) were emergency transfers, needing specialist review/intervention/escalation of care. Of the emergency transfers, 28% (n=8) deteriorated quickly after the initial transfer and bounced back to the level 3 unit within four days of the initial transfer (TABLE 1). Two infants sadly passed away, one with necrotising enterocolitis (NEC) and the other with Escherichia coli sepsis.

TABLE 1 Emergency ‘bounce backs’ after acute deterioration within four days of repatriation (n=8).
The most common reasons for elective re-transfers included:
- specialist review and management (37% of repatriations, FIGURE 2)
- planned investigations (12% of repatriations)
- procedures or central line insertion/removal (6% of repatriations).
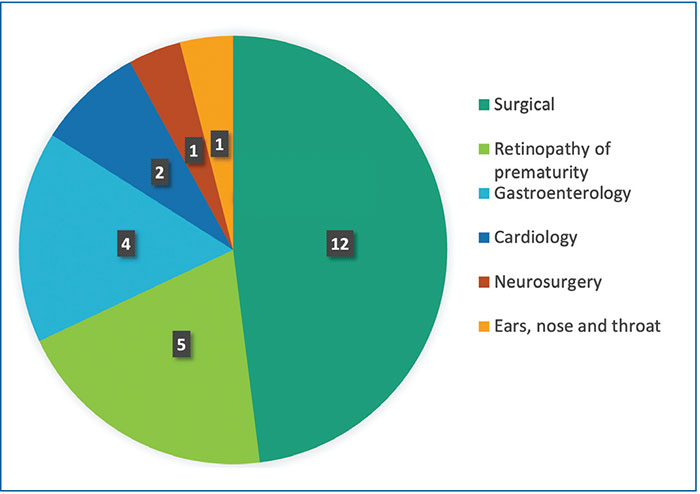
FIGURE 2 Elective transfers for specialist review and management: breakdown of cases (n=25) by discipline.
Conclusion
Immediate bounce backs are uncommon but tend to suggest more serious issues. Common causes, such as sepsis and NEC, are relatively unpredictable. Most return transfers are later and for less acute issues, which can be managed well in a way that maintains level 3 capacity by moving between units. Our data are reassuring as they show that immediate bounce backs are rare and appear to be due to unpredictable causes. This data should assist in repatriation planning for networks; networks should monitor rates in conjunction with the neonatal transport services.
Or read this article in our
Tablet/iPad edition
