

Maintaining quality of care through a pandemic and setting goals for future improvement
The National Neonatal Audit Programme (NNAP) was established in 2006 and continues to play an important role in driving and supporting improvements in neonatal care. The past two years have been a period of change for the NNAP, bringing a new data flow methodology, exciting opportunities to further develop the NNAP, and a new contract for the Royal College of Paediatrics and Child Health (RCPCH) to deliver the audit until 2025.
Sam Oddie
NNAP Clinical Lead, Consultant
Neonatologist, Bradford Teaching Hospitals
NHS FT
Rachel Winch
NNAP Manager, Royal College of Paediatrics
and Child Health
nnap@rcpch.ac.uk
It has also been a period of challenge for all those involved in delivering care and for service users. In March this year, the NNAP published its annual report on 2020 data1 – a period when societal lockdowns, limitations to parental access, staff shortages and general disruption to hospital services had the potential to significantly impact care delivery, and overall had a negative impact on families’ experience of it.
The report focuses on a wide range of process and outcome measures across the neonatal care pathway, from antenatal interventions to clinical follow up assessing development at two years of age. In general, the impression is that the quality of perinatal and neonatal care reported by the NNAP was well maintained and in some cases improved, despite the pandemic.
The latest NNAP annual report.
Key messages from the NNAP 2020
data report
- Adverse outcomes – bronchopulmonary dysplasia (BPD), necrotising enterocolitis (NEC) and infection – varied importantly across neonatal units and networks in 2020. For example, the proportion of babies with BPD varies by 11 percentage points between neonatal networks, and adjustment for background variables does not account for geographical variation. This likely represents unwarranted variation and an opportunity to change care to improve outcomes.
- Mortality in very preterm babies varies substantially (from one in 25 babies to one in 12 across neonatal networks) depending on where they are cared for, even when baseline risks are considered. This is unexplained.
- Despite the significant impact of COVID-19 on aspects of healthcare delivery in the period after March 2020, neonatal services have achieved high, and improved, rates of perinatal health promoting strategies such as antenatal steroid administration, antenatal magnesium sulphate administration, normal temperature on admission and birth of extremely preterm babies in a centre with a neonatal intensive care unit (NICU). However, variation persists between neonatal units and networks, demonstrating opportunity for further improvement.
- Implementation of deferred cord clamping (FIGURE 1) varies greatly between neonatal units and networks – ranging from 7.3% to 60.6% among networks, with higher levels of deferred cord clamping in NICUs. This is the first year of reporting this audit measure in the NNAP and rates of missing data are significant as well as results varying greatly between services.
- There has been no significant change in of the proportion of babies receiving breast milk, either at 14 days of age or at discharge from neonatal care in recent years. However, nationally, rates of breast milk feeding appear to have been maintained despite the COVID-19 pandemic. Low rates of breast milk feeding, variation by geography in use of breast milk, and variation within unit types has persisted over time.
- Restrictions on parents’ access to the neonatal unit imposed in response to the COVID-19 pandemic from March 2020 onwards may have impacted on parental consultation within 24 hours of admission and parents’ attendance on ward rounds. The rate of parental consultation has reduced by 1.2 percentage points compared to 2019, and the rate of improvement in parents’ attendance on ward rounds has slowed. However, variation in performance varies widely between neonatal units, and some units have been able to maintain high performance in these measures.
- Compliance with nurse staffing ratios set out in the service specification for neonatal critical care is improving. However, neonatal networks vary widely in the proportion of shifts staffed according to specification and fall far short of full compliance. Given the clear link between higher nurse staffing ratios and improved outcomes, nurse staffing remains a serious challenge for neonatal services.
- The rate of improvement in the delivery of medical follow-up at two years of age has been slow with a reduction seen in 2020, which may be due to the impact of the COVID-19 pandemic (FIGURE 2). Wide geographical variation remains in its delivery.
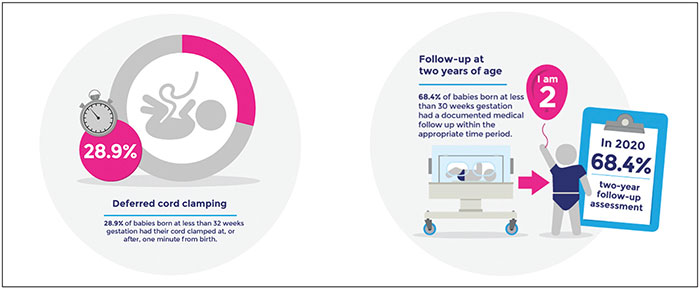
FIGURE 1 (left) Implementation of deferred cord clamping varies greatly between neonatal units and networks.
FIGURE 2 (right) The rate of improvement in the delivery of medical follow-up at two years of age has been slow.
What next for the NNAP?
The NNAP is operating under a new data flow methodology. The RCPCH now receives the data contained in the NNAP dataset directly from Clevermed Ltd, provider of the BadgerNet clinical system. Neonatal unit staff enter data onto the BadgerNet platform as part of routine care while a baby is present on the neonatal unit. The NNAP team receives and processes data that are solely required for care quality and service improvement in relation to the aims and scope of the NNAP. This new data flow methodology presents an exciting opportunity for the NNAP to explore opportunities for further use of the NNAP data, for example the possibility of linking to the Second Generation Surveillance System (SGSS) dataset held by the UK Health Security Agency for reporting neonatal bloodstream infection rates.
The NNAP has also been asked to develop more frequent repor-ting in the public domain, which presents both opportunities and challenges for the audit and the wider neonatal community.
Our goals for improvement
The RCPCH is delighted to have been commissioned by the Healthcare Quality Improvement Partnership (HQIP) to deliver the NNAP for a further three years until 2025. The NNAP has a Healthcare Improvement Strategy that will steer the work of the NNAP over the next three years, and aims to align as closely as possible with national ambitions and other programmes of work such as the Maternity and Neonatal Safety Improvement Programme (MatNeoSIP)2 in England, and the Maternity and Children Quality Improvement Collaborative (MCQIC), part of the Scottish Patient Safety Programme.
The strategy sets out three improvement goals that reflect existing national priorities and are consistent with quality improvement ambitions. They are described over a 10-year time frame, with specified year-on-year ambitions:
- Reduce the mortality difference between the networks with the highest and lowest rates of risk adjusted mortality (4.5% based on 2019 results) by 0.4% per year over a 10-year period.
- For babies born at less than 32 weeks’ gestation, increase the proportion receiving all measured elements of the MatNeoSIP perinatal optimisation plan by 2% per year over a 10-year period based on an estimated baseline rate of 35% observed in the Scottish Patient Safety Programme.
- For babies born at less than 32 weeks gestation, reduce the proportion discharged home from neonatal care having experienced any serious complication of prematurity (including late onset infection, NEC, BPD and serious preterm brain injury) by 1% per year over a 10-year period (baseline rate to be established).
To achieve these goals, the NNAP has set out a series of supporting objectives, and approaches to stimulating healthcare improvement, which include:
- High quality data outputs that identify areas for action and support stakeholders’ improvement initiatives.
- Sharing best practice and quality improvement resources.
- Collaboration and engagement with regional and national initiatives.
- Parent and public engagement.
Supporting services to reduce health inequalities in neonatal care
Ensuring equity of access, delivery and outcomes in health care has become an area of increased focus in recent years and the NNAP intends to further develop its reporting to better support tackling healthcare inequalities at a local, regional and national level.
An important first step to providing the data to do this is ensuring that key data items are complete within the NNAP dataset to enable us to report NNAP results by ethnicity and deprivation index in a meaningful way. Within our 2022 data quality and completeness reports, we will be including the completeness of ethnicity and postcode fields back to neonatal units and networks to encourage better data entry in these areas.
How can you use the NNAP to support your local and regional improvement?
There are a range of things that audit participants can do to improve their NNAP results. Firstly, it’s important to raise awareness about the audit. NNAP Online is open-access and provides a wealth of audit data. Information at both unit and network level can be downloaded in a range of formats. Individual unit posters showing progress against 12 of the audit measures can be displayed in the neonatal unit, as well as a poster that units should adapt to indicate their action plan to address these results.
The NNAP also produces a parent guide to the annual report called Your Baby’s Care, which provides more detail about the 12 audit measures highlighted in the unit posters. All neonatal units in England and Wales have been sent hard copies of the unit posters and Your Baby’s Care, and Welsh units have also been sent these documents in Welsh. These documents can be very helpful to neonatal staff when talking to parents about the NNAP. In addition, NNAP Online and quarterly reports can indicate improvement opportunities.
QI Central3 is a dedicated quality improvement (QI) website that features a range of case studies focussing on audit measures. Furthermore, the British Association of Perinatal Medicine (BAPM) has QI resources including toolkits focussed on NNAP measurement areas.
Or read this article in our
Tablet/iPad edition
