

Psychosocial support provision for parents: an audit of UK neonatal units
Having a preterm birth and/or a sick infant that requires neonatal care is an emotionally traumatising event for parents. This is due to issues such as parent-infant separation, concerns for infant viability and the technological nature of the neonatal unit. It is argued that neonatal units should provide a varied and sustainable programme of psychosocial support for parents during the infant’s stay and after discharge. However, currently there is a paucity of knowledge about what type and range of support is provided within neonatal care. In this article we report on an audit of facilities, services and support that could address parents’ psychosocial support needs in UK neonatal units.
Gill Thomson
Professor in Perinatal Health
GThomson@uclan.ac.uk
Rebecca Nowland
Research Fellow
Claire Feeley
Honorary Clinical Reader
Maternal and Infant Nutrition and Nurture Unit, School of Community Health and Midwifery, University of Central Lancashire
Background
Parents of premature (<37 weeks’ gestation) and/or sick infants who require neonatal care can experience high levels of poor mental health.1-3 This can be due to issues including early and repeated separation from their infant and fears about their infant’s health, development, or survival.4 A survey study undertaken by Bliss with 589 parents whose infants required neonatal care found that 80% of parents felt their mental health had been affected, with 35% reporting their mental health to be ‘significantly worse’.5 Twenty-three per cent of respondents went on to be diagnosed with anxiety, and 16% diagnosed with post-traumatic stress disorder (PTSD) after their time on the unit.<>sup>5 Parenting premature and/or sick babies after discharge from neonatal care has also been described as challenging, time consuming and disruptive;6 with parents reporting ‘falling apart’ at the time of discharge, often associated with leaving the safety of the neonatal unit.7 As poor parental mental health has negative implications for infant developmental outcomes,8 the need for appropriate psychosocial support is a key public health concern.9
It is argued that neonatal units should provide a varied and sustainable programme of psychosocial support for parents both during the infant’s stay and after discharge.9,10 A multidisciplinary working group (comprising professional organisations and parents who had experience of neonatal care) convened by the US National Perinatal Association (www.nationalperinatal.org) recommends interventions such as family-centred care, flexible visiting policies, continuity of carer, peer support, and readily available support from mental health and interdisciplinary professionals.9 However, apart from one published audit of facilities for parents’ emotional needs in Sweden,11 there is a lack of knowledge about the types and range of support provided to parents within neonatal care. We aimed to address this knowledge gap by conducting an audit of facilities, services and support that could address parents’ psychosocial support needs in UK neonatal units.
Methods
Audit development and distribution
An online audit was distributed to UK neonatal units during July 2020 to February 2021. The audit was developed based on existing literature11,12 and feedback from five professionals/academics working in the area. Audit questions were designed to capture units’ facilities and services offered to parents during their infant’s stay and after discharge, and whether the support was provided to ‘all’ or ‘some’ parents. Questions included:
- options/policies for parents to stay on the unit
- whether and how parents’ mental health needs were identified
- whether parents were able to access support from psychologists, counsellors, peer supporters or for their religious/cultural needs
- provision of any parent-led groups or information-based sessions
- whether the unit had any parent-based forums (ie Facebook groups).
Most questions were multiple choice; open text options were included. An online secure platform was used (Qualtrics XM) for audit dissemination. An introductory email and link to the online audit was distributed via existing networks, neonatal leads and social media.
Ethics
The study was reviewed by the Chair of the Health Ethics Committee at the lead author’s university (project number: 0042).
Data analysis
All completed audits were uploaded into SPSS v27 statistical software and quanti-tative data were presented as frequencies (percentages). Narrative comments were combined with the descriptive statistics and analysed using a basic thematic approach, similar to other audit-based studies.13
Findings and discussion
We received completed audits from 80 neonatal units (out of 181 units in the UK; 44.2%), completed by different staff including ward managers, matrons, consultant paediatricians and clinical psychologists. We received audits from units in all UK countries and all geographical areas in England (TABLE 1). Fifteen units (18.8%) were special care baby units (SCBUs), 26 (32.5%) were local neonatal units (LNUs), and 39 were (48.8%) neonatal intensive care units (NICUs). Comparing the study sample with national figures (SCBUs n=44, 24.3%; LNUs n=83, 45.9%; NICUs n=54, 29.8%) indicates an over representation of NICUs in the current sample. In the following sections we report on the audit data together with key supporting literature within four themes:
- Opportunities for parental presence
- Providing a therapeutic culture
- Types of psychotherapeutic support
- Parent-focused support.
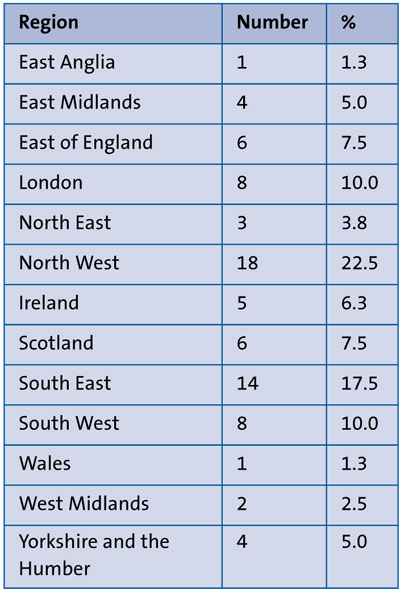
TABLE 1 Geographical regions of units completing the audit (n=80).
1. Opportunities for parental presence
Inclusive and flexible visiting policies on the neonatal unit are associated with physical, emotional and social wellbeing of parents and infants.14 Single family rooms are also perceived to offer an optimum standard of care.4 Our audit revealed that while most units provided family rooms (92.5%, n=74), they were only available for a small number of families. The number of family rooms ranged from one to 10, with most reporting 1-2 (and only two units citing 10). Furthermore, these rooms tended to be prioritised for parents preparing for discharge, parents who did not live close by, parents whose infant’s health was deteriorating, and, on one occasion, where ‘mothers who are trying to establish breastfeeding are encouraged to stay 24/7’ (LNU #12).
Just over 40% (n=33) of the units had accommodation nearby for parents to stay close to their infant (provided by charities – Ronald MacDonald houses, or on-site hospital options). However, some accommodation types were not inclusive due to being ‘fee paying’, or deemed not suitable for certain parents (ie not those who are ‘vulnerable, single or ill mothers, as it may not be appropriate’, NICU #8). Some accommodation could restrict parents’ access (eg ‘the entrance [to the accommodation] gets locked at 10pm’, NICU #7).
Overall, 65.0% (n=52) allowed parents to stay in the unit 24/7, thereby indicating that just over one third of the units had restricted visiting policies that limited the amount of parent-infant contact. Some respondents referred to how their units had (or intended to purchase) ‘comfor-table’ or ‘reclining’ chairs, or ‘camp beds’ at each cot space to enable parents to stay 24/7. Those not able to offer this facility often attributed this to a lack of physical space on the unit, for example, ‘there is just 76cms between the cots at our special care unit […] so very challenging’ (SCBU #15). Some also referred to overnight stays as being discouraged, for example, ‘parents are not able to sleep well’ (SCBU #15).
The spatial as well as attitudinal reasons underpinning restricted visitation policies and access to accommodation types confers with wider literature in that parent-infant proximity on neonatal units is dependent on individual, cultural and organisational level factors.15,16
2. Providing a therapeutic culture
Only 30.0% (n=24) of units had neonatal staff that were trained in psychological approaches, and from qualitative comments this generally involved specialist training being accessed by specific staff members, such as: ‘a degree module in counselling’ (LNU #11). Only two respondents referred to all/key staff being trained: ‘all staff, including cleaners, trained in basic counselling/active listening, yearly update’ (LNU #51), thereby aligning with the whole system approach advocated within mental health.17
Fifteen percent of units (n=12) used validated questionnaires or screening tools to assess parents’ psychological needs, administered by various professionals (ie. a clinical psychologist, member of the family support or perinatal mental health teams) and at different time frames, such as admission only, or on occasion ‘at any point in their journey’ (NICU #66). Overall, this general lack of consideration of parent mental health is out with current UK guidelines. This guidance states (albeit within a maternity rather than neonatal context) that women should be asked about their mental health and emotional wellbeing at every interaction with a health professional throughout pregnancy and the first year after birth.18,19
The Better Births maternity transformation agenda and the NHS long-term plan19,20 recommend continuity of carer and personalisation within maternity care. However, this emphasis is not apparent within neonatal care; only 52.5% (n=42) of units gave ‘all’ or ‘some’ parents/families a named neonatal staff member to contact, which reduced to 43.8% (n=35) of units post-discharge. Wider research indicates that dedicated neonatal staff can help build trust between parents and staff, which in turn can help parents to feel valued, included and significant in their infant’s life and care.10 However, audit data revealed that named staff would generally only be allocated to parents in complex situations, such as when the family has safeguarding issues, or the infant has congenital or life-limiting conditions. Furthermore, on occasion the named nurse was a role rather than person-specific, for example, ‘there is a named nurse for every day of the week, which the parents can see if required’ (NICU #50). Alternatively, the parents may be told to contact teams (eg ‘the neonatal community outreach team’) or to speak to ‘any staff member’ (LNU #1) at any point post-discharge. These results thereby indicating that even if parents were allocated what was perceived to be ‘dedicated staff’, it would not necessarily facilitate relationship-building.
3. Types of psychotherapeutic support
The different types of psychotherapeutic support available for parents while their infant was in neonatal care and after discharge are displayed in TABLE 2 and TABLE 3 respectively, and discussed in more depth below and in the following section.
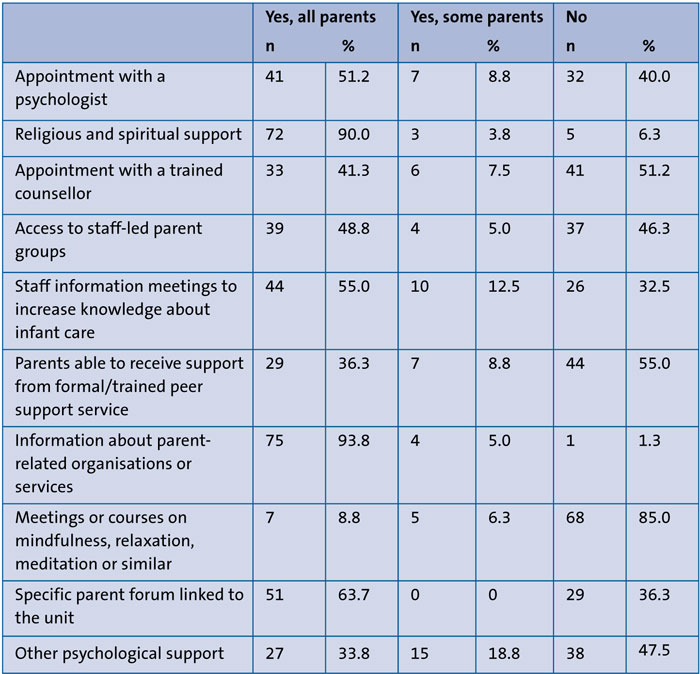
TABLE 2 Psychosocial support within the neonatal unit.
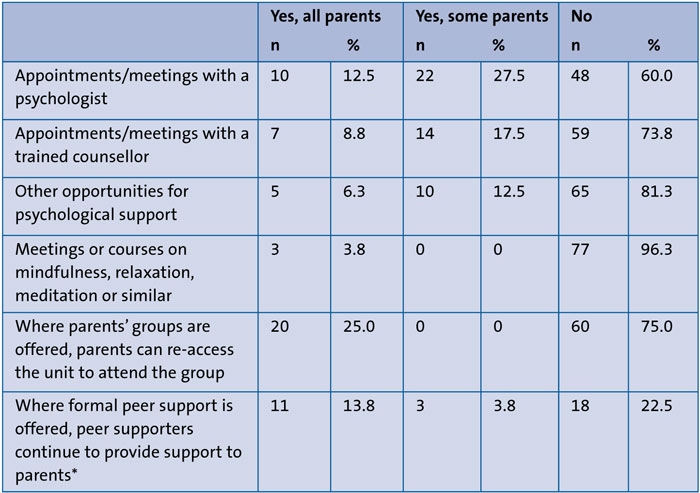
TABLE 3 Psychosocial support available after infant discharge. *48 units (60%) reported not having peer supporters.
During the infant’s hospitalisation, 60.0% of units (n=48) offered all/some parents an appointment with a psychologist (eg a hospital-based psychologist, psychotherapist, trainee clinical psychologist) and 48.8% (n=39) offered all/some parents opportunities to access counselling (eg bereavement counsellor, perinatal mental health team); with this provision reducing to 40.0% (n=32) and 26.3% (n=21) after discharge, respectively. Some respondents referred to offers of comprehensive provision such as a women’s health counsellor, who could offer parents ‘up to six sessions and then refer on if needing longer term support’ (NICU #14). One unit also had a flexible approach of parents being ‘able to call on a Friday’ to speak to a psychologist (LNU #30). Whereas others highlighted that even when this type of support was available, it was limited to, for example, one, two or three days a week, meaning that provision was restricted to those most in need. Post-discharge follow-up was also only generally offered to those who had received support during their infant’s admission, which for one unit involved an outpatient clinical psychology service ‘for infants assessed as having complex physical health care needs and their families’ (LNU #37). The number of units unable to offer an appointment with either a psychologist or counsellor was 25 (31.3%) during infant admission and 45 (56.3%) after discharge.
These findings highlight that despite positive evidence of psychotherapeutic interventions (such as psychological support and/or counselling) helping to reduce trauma and anxiety in parents of premature infants,21 large numbers of units do not offer this specialist support, particularly after discharge. This is likely to be due to resource implications.12
Religious support was the most widely available in 93.8% of units (n=75) for all/some parents during their infant’s hospitalisation and tended to be provided by hospital chaplaincy services. This support could be offered 24/7 or some units had an arrangement for a hospital chaplain or chaplaincy volunteers to visit on a regular basis, ie once or twice a week. Many respondents referred to how different faiths were supported by ‘non-denominational chaplains’ and ‘multi-faith chapels’, or by making ‘contact with someone from that faith or belief to arrange visits or whatever the parent requires’ (NICU #48). While a number of religious-based interventions have been evaluated for parents of premature infants, the interventions are heterogenous and the evidence-base is mixed.12 Moreover, these interventions only target those within a Muslim faith context,12 thereby suggesting that further research is needed.
Only 12 units (15.1%) offered all/some parents any opportunities to attend any meetings or courses on mindfulness, relaxation, meditation or similar during the infant’s inpatient stay, and only three units (3.8%) provided this support post-discharge. ‘Other’ opportunities for psychological support – provided by 42 units (52.6%) during hospitalisation and 15 units (18.8%) after discharge – included providing parents with wellbeing resource packs, scrapbooking, rewind therapy and debriefing sessions. However, as yet, there is little evidence (if any) of the effectiveness of such approaches for parental wellbeing.12,22
Overall, the variable level of psycho-therapeutic support across the units supports wider arguments about the postcode lottery of mental health care in the UK.23 Furthermore, while service provision often reflected the ethos of universal proportionalism,24 with more targeted psychotherapeutic support provided for parents who had specific needs, the gaps in parents being able to access suitable psychosocial support is highlighted.5 National standards for neonatal care in the UK recommend that all parents should have access to psychological and social support including a trained counsellor.25 Our findings highlight that many neonatal units are failing to meet these minimum standards.
4. Parent-related support
Forty-three units (53.8%) provided staff-led parent groups for all/some parents to access during their infant’s hospitalisation. These groups were provided at varied intervals (eg weekly, fortnightly, four times a year) and facilitated by different staff members (eg nursing staff, infant feeding leads, psychologists/counsellors, chaplaincy service, medical/allied health professionals and/or parenting representatives). Only 20 units (25.0%) offered parents the opportunity to re-access the parent group after discharge.
Some groups were designed for parents facing specific issues, such as cystic fibrosis. Others were offered as part of the unit’s wider commitment to family-centred care, for example, ‘with slots for medical consultant, pharmacist and nursing staff to have tea with parents in the family room’ (LNU #11). While a few respondents described the group’s purpose as offering catch ups, more commonly they were designed to facilitate specific types of support (ie psychology-led discussions, meditation, crafting, baby massage). On occasion, this could involve a rolling programme of information, for example, ‘coping on the neonatal unit, caring for your baby, preparing for home, feeding support, sibling support and first aid’ (LNU #51). Respondents on units that currently did not offer groups also provided reasons as to why. These included efforts being ‘fizzled out’ due to poor attendance, the lack of space on the units to facilitate groups, or the individual who was the motivating force in facilitating the groups having left or ‘retired and no one else has taken over’ (NICU #34).
Over half of the units (n=54, 67.5%) provided information meetings to all/some parents, with this support provided on an individual rather than group basis. Respondents detailed how these meetings would often involve specialist instruction such as ‘physiotherapist – developmental awareness, clinical nurse specialist – respiratory information re. home oxygen, etc’ (NICU #2). They could encompass information on caretaking behaviours, parent wellbeing, infant feeding, information about their baby’s needs and general baby care. On some occasions, meetings were regularly provided (such as discharge planning) or were informally provided based on need. One respondent explained how there were ‘resource boxes with teaching aids available to staff at all times’ to provide needs-led care (NICU #7). Another described a more unique service of daily ‘walk about sessions’ by different professionals (NICU #20) to offer information as needed.
Overall, while the effectiveness of staff-led groups and information sessions on parental wellbeing outcomes is lacking,12 there is a wealth of evidence that highlights that parents value targeted support to increase their knowledge and caretaking behaviours over the course of the infant’s hospitalisation.26,27
Thirty-six units (45.1%) enabled all/some parents to receive support from peer support organisations, and/or hospital-based peer provision (whereby parents who have had a premature/sick baby are trained to provide support to others). Moreover, almost all units (n=79, 98.8%) provided all/some parents with information about parent-related organisations or services. This involved literature (ie packs, leaflets, contact cards) being handed to parents and/or posted on unit notice boards. One unit gave parents ‘an iPad and those apps [from support organisations] are installed’ (NICU #69). In only 14 units (17.6%) were parents able to continue to receive peer support after discharge, such as via community groups, online support or via telephone.
Evidence highlights that support from trained peer supporters (as well as informal opportunities for parents to connect during staff-led groups) can relieve parents’ anxiety and help parents gain parenting skills.28-31 Parents value opportunities to talk to others who understand their lived realities and who can offer reassurance to normalise their emotional responses.29,30,32 One respondent also reflected that a key benefit of veteran parents re-accessing the staff-led group was: ‘to chat to parents who have been through the journey’ (NICU #16). As over half the audited units (n=44, 55.0%) did not provide formal peer support, this may reflect wider insights of peer support being difficult to implement due to mistrust between peers and professionals, recruitment and/or funding issues.7 Fifty-one units (63.7%) had a specific parent forum linked to the unit, which may help to bridge this gap. These were generally closed or open Facebook groups (although a few also referred to WhatsApp, Instagram, Twitter and/or email groups), where parents could share news, pose questions and offer peer support. Although, evidence highlights the benefits of parents being able to select options (face-to-face or online peer support) that suit their individual values and needs.33
Strengths and limitations
The strength of this work is that it is the first published UK audit of psychosocial support, highlighting the types, range, and gaps in provision for parents. While only approximately 44% of UK neonatal units are represented, we did achieve geographical coverage and this work can serve as a benchmark for comparison with different contexts and countries. A limitation is that this work offers baseline data only; further research is needed to determine the optimum, or minimum level of standards that should be achieved. Finally, while the audit was issued during the COVID-19 pandemic, to the best of our knowledge the responses reflect usual care with some respondents indicating that some services (ie parents’ groups and access to units) were restricted during this time.
Conclusion
Parents of premature and/or sick infants can experience poor mental health and they should have access to psychological and social support both during and after the infant’s hospitalisation. Our study is the first UK audit to explore psychosocial provision provided to parents in neonatal care. Our work highlights that all the audited units provide parents with ‘some’ type of psychosocial support. However, the scope and range of support varied considerably with the most common offers relating to chaplaincy services and providing information about parent-related organisations or services. Key gaps regarding visitation policies/opportunities, routine mental health screening, psychological support with a trained professional and access to formal peer support were noted. Consistently, psychosocial support was poor following the infant’s discharge home. Further mixed-methods research to identify outcomes in parents who have access to different and varying levels of support could help to recognise what works for different groups of parents in different settings, and help to identify universal standards of best practice.
Author contributions and funding
GT conceived the original ideas for the study; GT/CF developed and distributed the survey; GT/RN analysed the data set; all authors contributed to writing the manuscript. Funding for this study was provided by internal funds: a THRIVE small grant award, and LIFE writing group award.
Acknowledgement
The authors would like to thank Raeesa Jassat for her help with audit distribution.
Or read this article in our
Tablet/iPad edition
- While most neonatal units provide family rooms and/or nearby accommodation, these options are limited and often restricted to specific parents.
- Only 15% of units use any screening tools to assess parents’ psychological needs during infant admission.
- Over 30% of units do not offer parents appointments with a psychologist or counsellor, thereby failing to meet recommended minimum standards.
- There is a paucity of psychosocial support available to parents following their infant’s discharge from the unit.
Also published in Infant:
