

Using servo-control as a part of a normothermia bundle during delivery room resuscitation of preterm infants
Rhianna Netherton
Paediatric Trainee
Amitava Sur
Neonatal Consultant
amitava.sur@elht.nhs.uk
Jasim Shihab
Neonatal Consultant
Lancashire Women and Newborn Centre, Burnley
What is known about this topic?
- For each degree of temperature <36.5°C, mortality in the newborn population increases by 28%.1
- Premature infants are more susceptible to hypothermia and adverse outcomes, such as mortality and necrotising enterocolitis, are associated with hypothermia.2
The problem
Hypothermia has known correlation with neonatal mortality, especially among preterm infants. Maintenance of normothermia (36.5-37.5°C) is one of the key quality indicators of optimal neonatal care. The data in 2018 obtained from the National Neonatal Audit Programme (NNAP) for the Lancashire Women and Newborn Centre (LWNC) showed that only 67.9% of infants born at <32 weeks’ gestation were normothermic on admission. Comparing this to the national average of 70.3% highlighted the importance for practice change.
We set out to implement a ‘normothermia bundle’ including use of servo-controlled thermoregulation during resuscitation for preterm infants in a tertiary neonatal unit. The other key elements in the bundle were:
- Awareness around hypothermia through educational leaflets and posters in the maternity and neonatal units and delivery room areas.
- A visual aide memoire on the resuscitaire and resuscitation trolleys prompting to check temperature at five-minute intervals during resuscitation (FIGURE 1).
- iDesignation of a ‘temperature champion’ for all high-risk resuscitations.
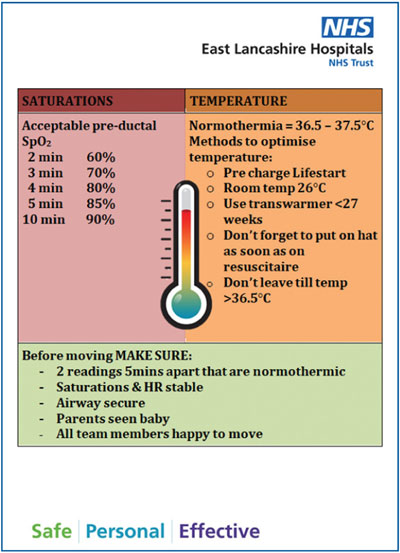
FIGURE 1 The visual prompt of thermo-regulation awareness for the delivery room team.
The introduction and implementation of the bundle was carried out with weekly task training simulation sessions and short educational sessions during morning handovers (capsule teaching).
Most units in the UK use manual control of temperature during resuscitation, which depends on a radiant heat source or an exothermic heating mattress (a transwarmer) to maintain normothermia. One of the problems with manual control is incidence of hyperthermia (a temperature >37.5°C), which is also associated with adverse outcomes in the preterm cohort.3
Servo-control utilises an electronic feedback system that functions as a thermostat to maintain a constant temperature at the site of a thermistor probe (usually on the skin over the abdomen) by regulating the heat output of an incubator or radiant warmer.
There is no clear evidence to recommend use of servo-control during resuscitation over manual modes, although the Neonatal Resuscitation Program (NRP) recommends its use.4 There is a report on the feasibility of using servo-controlled mattresses in preterm infants during transport.5
Aims of the project
- To reduce the number of infants born at <32 weeks’ gestation being admitted to the neonatal unit with a temperature <36.5°C to zero, within 12 months of initiation of a quality improvement (QI) project.
- To reduce the percentage of infants having a temperature >37.5°C to less than 5%.
- To devise a new standard operating protocol (SOP) for thermoregulation during delivery room resuscitation for preterm infants, to include the use of servo-control.
Making a case for change
The QI initiative was proposed during departmental discussion of NNAP data measures. Two named consultants volunteered to lead on this. One senior nurse educator, one senior neonatal registrar and two foundation year trainees were part of the core group with different roles in their capacity. This was registered as a project under the trust Quality and Safety Board.
Improvements
A driver diagram was created (FIGURE 2), which included three separate projects using multiple ‘plan do study act’ (PDSA) cycles and focusing on three main drivers:
- environment
- human factors
- equipment.
Environment
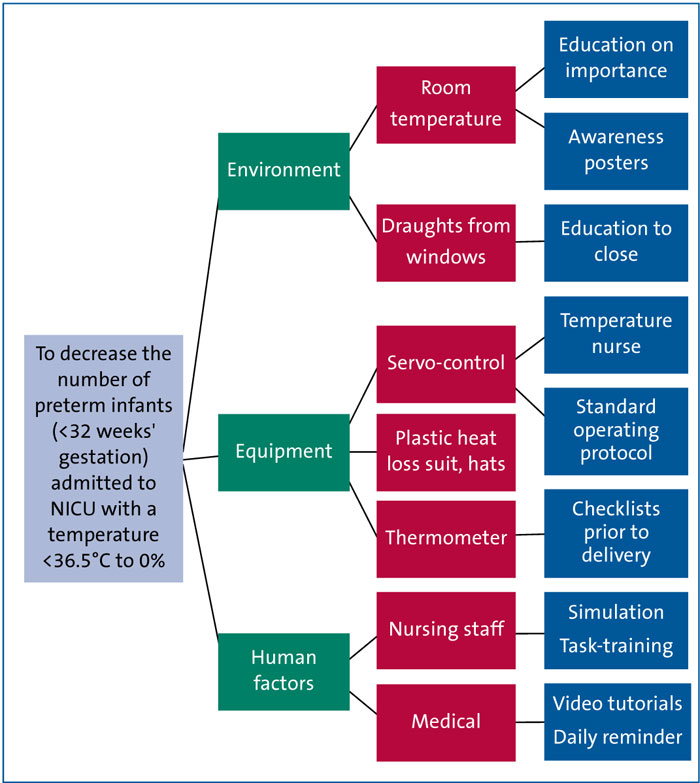
FIGURE 2 The driver diagram.
Over a 14-month period preceding the initiative, the average temperature of all delivery areas was 21.6°C. Highlighting the importance of environmental temperature involved disseminating information about ideal delivery room temperature (26°C), visual aide memoirs, posters and staff training. Optimising the delivery area temperature required three stages of PDSA cycles; an audit after the third cycle demonstrated significant improvement, with the average temperature across all delivery areas increasing to 25.4°C.
Servo-controlled equipment
The existing version of the delivery room protocol for resuscitation advocated use of thermal adjuncts (eg transwarmer mattresses and customised plastic bags) for all preterm infants, but did not have an algorithm for thermoregulation and did not advise use of servo-control. A new SOP for thermoregulation during delivery room resuscitation for preterm infants was devised, which included the use of servo-control.
A process map of thermoregulation was produced in the form of a flow diagram with specific emphasis to the allocation of the role of the temperature champion who was equipped with a thermal care checklist. This was shared among all relevant healthcare professionals via teaching, multiple simulation sessions and daily reminders. A transwarmer was used during delayed cord clamping of one minute. Once the infant was brought to the resuscitaire, a temperature probe was immediately placed on the right axilla by a dedicated ‘temperature nurse’ and the resuscitaire was switched to ‘baby mode’ with a set temperature of 37°C.
The detailed steps in the checklist are outlined in FIGURE 3. The entire QI project was carried out in two separate, but overlapping, phases with distinct areas of focus over a 14-month period:
- Phase 1 - optimising delivery room temperature
- Phase 2 - servo-control training and use.
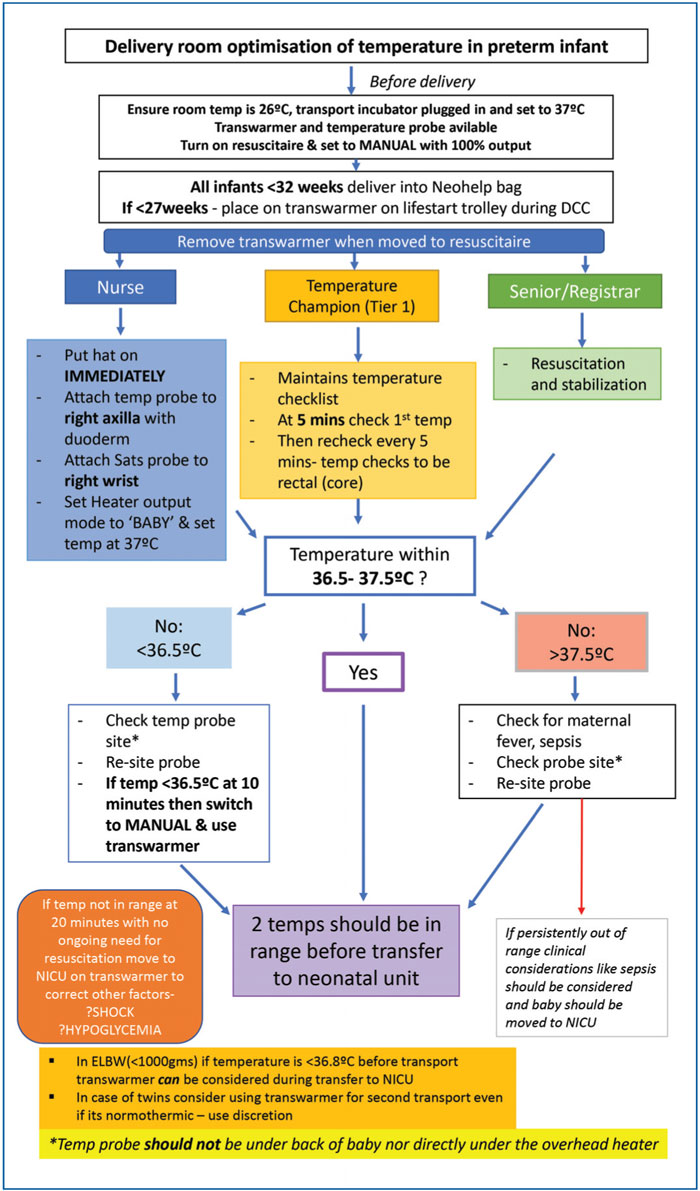
FIGURE 3 The standard operating protocol for delivery room thermoregulation for preterm infants. Key: DCC=delayed cord clamping; ELBW=extremely low birth weight.
Outcomes
Initial data collected over a feasibility period of three months showed that 100% of infants (n=39) born at <32 weeks’ gestation who were admitted to the unit, had a temperature that was within range prior to transfer. Of these, 81.2% were normothermic on admission to the unit (temperature taken within one hour). It was felt that most of those infants who were thermoneutral in the delivery room but were hypothermic on admission to the neonatal unit had lost heat during transport. Infants are transferred from the delivery area to the neonatal unit, which is situated a floor below, in a transport incubator. It was recommended as a learning process that those infants who have a temperature of 36.5°C at the point of transfer could benefit from a transwarmer mattress during this journey.
Staff were given further training on the use of servo-control and the following six months of data showed that 91.8% of <32 weeks’ gestation infants admitted to the unit were normothermic on admission and only 6% were hyperthermic on admission (FIGURE 4).
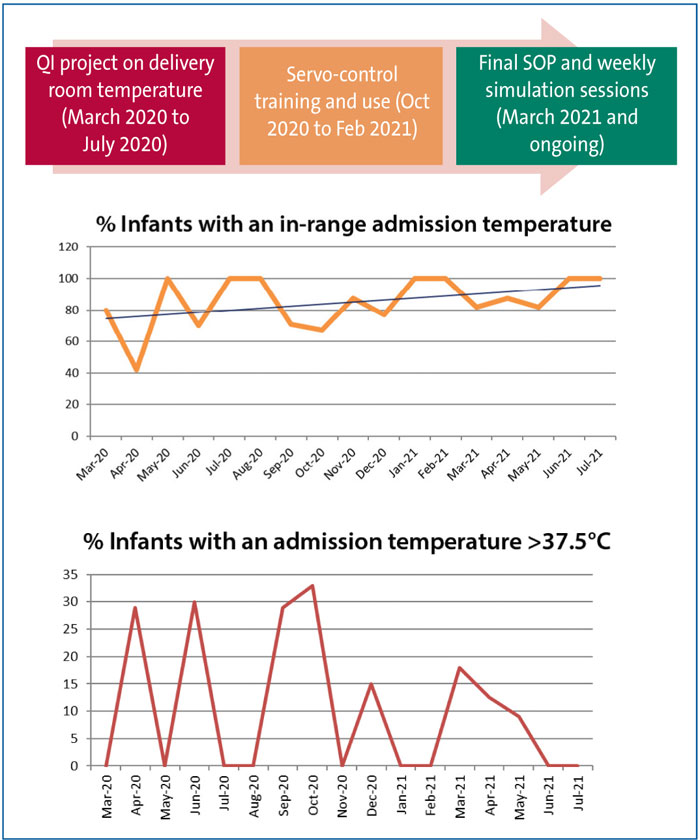
FIGURE 4 Run chart for the thermoregulation data for preterm infants admitted to the neonatal unit during the period March 2020 to July 2021 (n=147).
Learning and next steps
The improvements demonstrated were a result of a robust QI process and intensive multidisciplinary simulation. The results were shared among the network data and quality group.
We encountered challenges around compliance with maintaining the environmental temperature at 26°C, due to lack of availability of temperature probes in all delivery areas and some hesitancy in using servo-control.
Hypothermia during transport from the delivery suite to the neonatal unit was identified as an area for improvement; we are addressing this by the selective use of transwarmer mattresses.
As was evidenced during the data analysis, the initial improvements following the introduction of phases 1 (delivery area temperature optimisation) and 2 (training on servo-control) were encouraging but not steadily sustained. It was only after the final SOP was developed and the repeated training sessions on awareness and equipment carried out, that we could enter the sustenance phase of the QI project. This project is currently in the sustenance phase and we are monitoring monthly data for admission temperatures of all preterm infants.
Conclusions
- Servo-controlled mode during resuscitation is feasible and effective in maintaining normothermic range.
- A bundle approach addressing key areas is more effective in improvement than isolated measures.
Or read this article in our
Tablet/iPad edition
