

A dorsal urethral cyst in a newborn:an image case report
Parameatal urethral cysts are benign congenital lesions of the penis that are extremely rare in the newborn period. This article presents the case of a term infant with glanular hypospadias and a cystic lesion extending from the glans penis.
Sarah Arthur
Paediatric Registrar
Severn Deanery
Pieter Van-Hensbergen
Neonatal Consultant, Musgrove Park Hospital, Somerset NHS Foundation Trust
The case
A term male neonate was found at birth to have a cystic lesion extending from his glans penis. He was a low risk preg-nancy with no significant antenatal history born by spontaneous vaginal delivery.
He had a normal systemic examination with a glanular hypospadias. The cyst was dorsal to the urethral opening (parameatal) and measured 0.8mm (FIGURE 1a AND 1b). The infant showed no signs of discomfort when the lesion was examined. The urethral opening appeared crescent and slit-like (FIGURE 1c). The medical team was concerned there may be external compression of the urinary system, however, no features of obstruction were present on the bladder scan or clinically. The infant passed urine at exactly 24 hours of age with a normal stream.
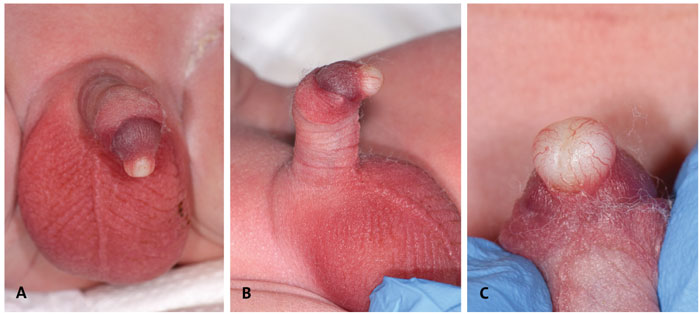
FIGURE 1 (A) The urethral cyst arising from the dorsum of the glans penis. (B) Glanular hypospadias with the dorsal urethral parameatal cyst. (C) A crescent urethral opening with the parameatal cyst dorsal to the urethra.
On day 2, the cyst spontaneously ruptured. The baby was referred to the urology team for further assessment of the hypospadias and to ensure no recurrence. When reviewed at six months of age, the urologists consented for a meatoplasty due to meatal stenosis. There was no recurrence of the cyst at this time.
Discussion
Glanular hypospadias is a relatively common congenital condition in which the opening of the urethra is located on the head of the penis, but not at the tip. However, parameatal cysts are rare and therefore maybe unfamiliar to paediatric, neonatal and midwifery staff. There are no reports of direct urethral communication and obstruction is a rare feature.1 It is extremely rare to have other associated congenital abnormalities; only one previous report has described hypospadias.2
Embryologically the urethra is fully formed by the fourth month of gestation. The urethral groove is endodermal in origin and elongates parallel to the growth of the penis. The urethral tip consists of ectodermal cells and develops in the glans, these cells canalise to connect with the rest of the urethra.3 Urethral cysts commonly present on the ventral surface; theories include blocked paraurethral ducts and persistence of cystic spaces during preputial development.4-6 In the case presented here, the cyst was dorsal in origin. Urethral cysts largely present outside of the newborn period and are mainly asymptomatic. In a study of 69 children, 42% were managed non-operatively and, of 22 responders to follow up, 27% spontaneously resolved, 68% improved or stabilised, and 95% remained symptom free.1 In the newborn presentation, urethral cysts may recur, maybe associated with other abnormalities and surgical excision maybe required. Reassurance to parents with discussion or referral to urologists is therefore recommended.
Parental consent
Written consent for publication was obtained from the parent of the patient.
Or read this article in our
Tablet/iPad edition
- Parameatal cysts are rare and maybe unfamiliar to paediatric, neonatal and midwifery staff.
- A parameatal cyst with associated hypospadias in newborn babies is extremely rare.
- Referral to a urologist may be necessary.
