

A welcome result of an unwelcome virus? Evaluation of video consultations within a neonatal service
The recent pandemic has necessitated the use of video consultations in order that babies can receive timely follow-up after discharge from the neonatal unit, while avoiding the risks associated with travel and social mixing during an in-person attendance at clinic. We analysed parental and clinician perceptions of the service delivered using the newly implemented ‘Attend Anywhere’ video consultation service. Video consultations are satisfactory to parents and can safely meet the needs of appropriately selected patients. The video consultation system can be utilised for a variety of interactions between neonatal staff and parents and in addition has benefits at a strategic and environmental level.
Jenna Deeming
Neonatal Registrar
jenna.deeming@mft.nhs.uk
Catherine Armstrong
Neonatal Registrar
Ngozi Edi-Osagie
Neonatal Consultant
St Mary’s Hospital Neonatal Unit, Manchester University NHS Foundation Trust
Traditionally neonatal follow-up clinics are held face-to-face in hospital settings by consultant neonatologists. In response to the COVID-19 pandemic in 2020 the NHS undertook a rapid rollout of telemedicine video consultations to reduce face-to-face appointments. Within the neonatal service at Saint Mary’s Hospital, we embraced the use of ‘Attend Anywhere’ telemedicine clinics and evaluated the experience of families and clinicians that used the service.
Background
Neonatal clinics are used to assess the growth, development and general health of babies who needed neonatal care at birth, and allow parents a forum to voice concerns they may have regarding their child. NICE (National Institute for Health and Care Excellence) guidance1 recommends enhanced developmental support and surveillance for children born at <30 weeks’ gestation and for those born at 30-36+6 weeks’ gestation with additional risk factors: a brain lesion likely to be associated with developmental problems, grade 2 or 3 hypoxic ischaemic encephalopathy, neonatal bacterial meningitis or herpes simplex encephalitis in the neonatal period. Within NICE guidance a minimum of two face-to-face follow-up visits in the first year and at two years’ corrected gestation are advised.
The use of telemedicine within neonatology is not widespread. At the start of the COVID-19 lockdown, the Liverpool Neonatal Partnership implemented a telemedicine service in which ‘robots’ were introduced on the neonatal unit, allowing consultants isolating at home to continue to provide a clinical service via a virtual consultation.2 Telemedicine has been used successfully within retinopathy of prematurity screening programmes3,4 and in addition to routine care on discharge,5 but the move to telemedicine video consultations for neonatal follow-up was unprecedented and its acceptability to families and clinicians unknown.
The system
Attend Anywhere is an online video consultation system that originated in Australia and was first utilised by NHS Scotland in 2016 before being rolled out across the UK during the COVID-19 pandemic.6 It allows patients to consult their healthcare professional via a video call from any location where they have an internet connection. Patients do not need an account or to download any special software and several mobile networks offer access to the portal without any charge. Reported benefits of the Attend Anywhere platform include reclaiming of travel and waiting time, saving money, reduce waiting times, optimised use of physical space, increased convenience and reduction of carbon footprint.7
The process
A standard operating procedure was developed and patients who were suitable for a video consultation were identified by their consultant. Parents were then contacted via telephone and, if they agreed to a telemedicine clinic, sent an invite to have their consultation via Attend Anywhere. Details of how to test their device, access the platform and what to expect were also sent. If an interpreter was required, this was booked and an invite also sent to the interpreter in order to undergo a joint appointment. Prior to the appointment, the baby’s weight and head circumference were measured in the community by the health visiting team, with the results sent on to the responsible consultant.
During the consultation, the clinician, patient, parents and any other additional family/interpreters ‘attended’ clinic from their individual locations. If parents lived at separate addresses, the same link could be used for multiple people to be present for the consultation. The clinicians were responsible for adhering to patient confidentiality, having access to and maintaining medical records and results, and leading the consultation. Following the consultation, a clinic letter clearly stating it was a video consultation was dictated and approved within five working days, as per departmental standards.
The feedback
Immediately following the appointment, families were asked to complete a feedback survey of their experience of a video consultation and the Attend Anywhere platform. After several months of use, clinicians completed a similar feedback survey based on their use of video consultations.
Family results
There were 54 family responses following the consultations, with overwhelmingly positive feedback. Regarding the use of the Attend Anywhere system:
- 51/54 (94%) of families felt that it was ‘easy’ or ‘very easy’ to join the call (FIGURE 1)
- 52/54 (96%) rated their experience of joining the call as ‘positive’ or ‘very positive’.
The majority of families (96%) agreed with the system’s claim that time is saved in comparison to a face-to-face appointment, with only 1 (2%) family stating that a video consultation was much more time consuming.
When asked how the video consultation compares to a face-to-face appointment, 5/54 (9%) families rated video consultation as ‘worse’ (FIGURE 2).
However, despite those five families rating the service as worse:
- only one family (2%) felt that their needs had not been met during the video consultation
- 53/54 (98%) families felt likely or very likely to choose video consultation again in the future
- 51/54 (94%) families said they would recommend video consultation to a friend.
The vast majority of comments, where given, were positive with one respondent stating: “It was just like being at the hospital but not having to leave your home” (FIGURE 3).
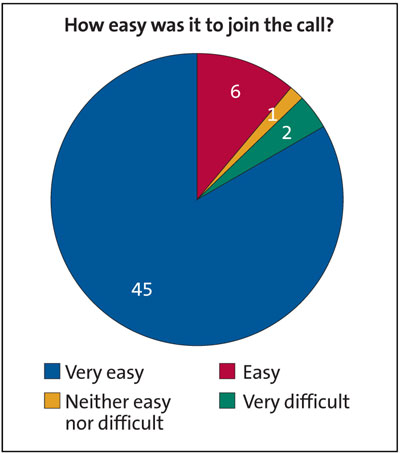
FIGURE 1 Parental responses to the question: how easy was it to join the call? (n=54)
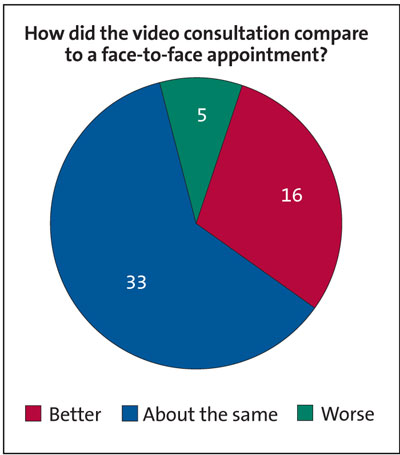
FIGURE 2 Parental responses to the question: how did the video consultation compare to a face-to-face appointment? (n=54)
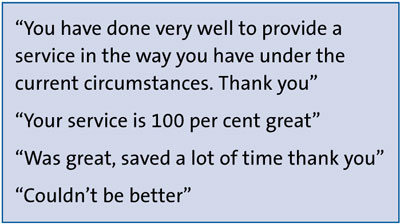
FIGURE 3 Examples of parental responses to the question: how could we improve this service?
Clinician results
Of the 10 completed responses, three clinicians had used video consultations prior to COVID-19, although the exact nature of this was not explored. In keeping with the families’ feedback, 80% of clinicians felt the system was ‘easy’ or ‘very easy’ to use.
The majority (60%) of clinicians felt that time was saved in comparison to face-to-face appointments. With regards to patients’ needs, the same majority of clinicians felt that they could ‘usually’ or ‘always’ be met using video consultations with just 10% feeling they could ‘never’ meet their patient’s needs (FIGURE 4).
Going forwards, 70% of clinicians felt that they were ‘likely’ or ‘very likely’ to use video consultation again.
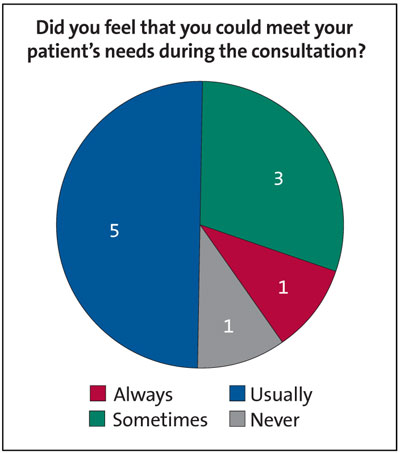
FIGURE 4 Consultant responses to the question: did you feel that you could meet your patient’s needs during the consultation? (n=10)
Discussion
The Attend Anywhere system is easy to use from the parent perspective, demonstrated by the overwhelmingly positive responses in terms of ease of use. Parents were almost unanimous in feeling that using Attend Anywhere was time saving when compared with face-to-face appointments. The potential for parents to feel that a virtual appointment is suboptimal when compared with a face-to-face appointment did not transpire to be the case in our study, with the vast majority of parents feeling that their needs had been met, and that they would choose a virtual appointment again in the future.
The ability for multiple family members to attend virtual consultations from different locations permits greater flexibility and allows the possibility of extended family attendance to support the parents during the consultation and enhance support networks after discharge. Further evaluation after a longer period of use of virtual clinics will assess whether this level of parental satisfaction is maintained, and whether the increased convenience and flexibility translates to fewer missed appointments and fewer A&E attendances, as has been noted in a previous Swedish study.5
Digital poverty was seemingly not an issue in our study population as 96% of parents reported it was ‘easy’ or ‘very easy’ to join the call; there were no negative comments as to difficulty accessing the required technology to utilise the Attend Anywhere system. However, parents were not specifically asked about issues around access to technology and, there will be a minority of families who do not have access to the devices required to participate in a virtual consultation. This could result in an inability to engage in the follow-up process, or anxiety and embarrassment in having to confide these issues to the medical team. One possible solution to this could be to add an ‘opt out’ option on discharge paperwork or the nursing discharge checklist whereby families could choose to have only face-to-face follow-up, without having to disclose their reasons for choosing this option.
Similar to parents, clinicians also found the Attend Anywhere system easy to use. The majority (60%) also found it to be time saving compared to face-to-face appointments. It is perhaps not surprising that a smaller proportion of clinicians than parents found virtual appointments to be time saving, as they are already based in hospital and do not have to factor in travel and parking times.
Although overall positive, consultants were not as convinced of their ability to meet their patients’ needs during a virtual consultation. This was in contrast to parents who felt that their needs had been met in all but one case. One explanation for this is the possibility of picking up new or unexpected findings during examination in a face-to-face consultation. Several text comments in the consultant responses alluded to an increased reliance on parents to report symptoms and make their own assessments of their child’s wellbeing and this seemed to cause anxiety on the part of the consultants. However, a previous study showing decreased A&E attendance after use of telemedicine consultations5 suggests that this anxiety may well be unfounded and it would be interesting to see if this finding is replicated in our population setting.
Clearly, there will be some patients who are unsuitable for a virtual consultation, either due to their medical status or social circumstances. In order to create a robust system that enjoys the full confidence of the doctors using it, and most importantly one that is safe and meets the needs of the patient population, it may be necessary to design a protocol as a guide to which patients are, or are not, suitable for virtual appointments, and also mandates the use of a face-to-face appointment, for example, after every two virtual appointments.
Future analysis would be helpful to evaluate whether clinicians’ confidence in their ability to meet the child’s needs has evolved or changed with increased experience with the virtual system. Extending our analysis to assess the influence of use of virtual appointments on A&E attendances, GP attendances, or frequency of unplanned interactions with the community nursing team could provide supporting evidence as to whether increased use of virtual appointments impacts upon ability to identify new or worsening medical problems in a timely fashion, thus affecting patient outcomes.
The use of virtual appointments also has wider implications both for service provision and environmental impact. Use of a virtual clinic format is in theory, only limited by the time available to the clinicians facilitating it. As it does not require clinic rooms and waiting areas, across a trust it should allow for increased clinic capacity, thus improving waiting times. Going forward, the use of the Attend Anywhere system can also be widened to facilitate joint clinics with different specialties, and to incorporate discussions with parents and/or interpreters who cannot be physically present on the neonatal unit, for example, where a baby has been transferred to the tertiary centre before its mother has been transferred from the local unit.
A virtual appointment system is not without impact on our community-based colleagues, ie health visitors and community nursing teams, and so long-term expansion of the virtual clinic system should be performed in consultation with them. Although in the short-term, it may be perceived as creating an increased workload (in the form of weight and head circumference checks), if there are beneficial effects in terms of a lessened need for emergency or ad-hoc presentations, this may result in a decreased workload for community teams.
Additional benefits of a virtual clinic system include a positive environmental impact, with fewer families having to travel to appointments.
Conclusion
Virtual clinics using ‘Attend Anywhere’ in neonatology are acceptable, time-saving and easy for families to access. Clinicians also view them positively and anxieties around the potential to meet patients’ needs and minimising missed oppor-tunities or diagnoses could be reduced with robust protocols for patient suitability. Further evaluation as to the impact of virtual clinics on clinic attendance, waiting times, and hospital reattendance will provide more evidence as to their effect on patient experience and service provision. Overall, virtual clinics may well be a welcome result of an unwelcome virus.
Author contributions
Dr N Edi-Osagie: idea for article and analysis of patient data. Dr J Deeming: idea and design of consultant feedback, data analysis, writing. Dr C Armstrong: data analysis, writing.
Or read this article in our
Tablet/iPad edition
- Virtual neonatal clinics are positively regarded by parents both in terms of ease of use, and ability to meet their babies’ needs.
- Clinicians regard video consultations positively, and concerns about potential for missed opportunities to pick up new information or diagnoses could be mitigated by guidance on appropriate patient selection and use of video consultation in conjunction with face-to-face consultations.
Also published in Infant:
