

Helping perinatal nurses cope with patient death
The death of an infant or maternal loss can be distressing for the staff that cared for them. Grief is an emotional reaction to loss and must be recognised among perinatal and neonatal nursing staff. Coping with stress and grief is important to enhance a nurse’s quality of life and decrease compassion fatigue and burnout in the workplace. This article considers the background and evidence of the problem, recommendations for change, and outcome influences. Healthy coping strategies are outlined, as well as ways in which staff and management can help each other to cope with the stress and grief of patient loss.
Catherine A. Pankonien
DNP, MSN-Ed, BSN, RNC-NIC
Assistant Professor
catherine.pankonien@msutexas.edu
Sandra M. Groth
DNP, MSN-Ed, RN, CNE
Assistant Professor
Midwestern State University, Wilson School of Nursing, Wichita Falls, Texas, USA
There are many stressful situations that nurses in critical care areas must work through to maintain effectiveness in their roles. In neonatal intensive care units these include:1,2
- high acuity patients
- staff/management issues
- patient families
- highly technological equipment
- quick clinical judgment during crises
- patient death.
For most people, death is challenging to cope with especially when it involves an infant or child. Compared to other losses, the death of a child is associated with a grief experience that is severe, long-lasting, and extremely complicated with features that fluctuate in intensity and duration.3,4 Thus nurses involved in making critical decisions and dealing with the death of an infant or mother, face high levels of stress and grief. The way a nurse deals with that stress and grief is personal to them.
Types of grief
Grief is the emotional reaction to loss.5,6 It is individualised based on the person experiencing it and the value of the loss to them. Grief may not be openly shared or acknowledged. Types of grief include anticipatory grief, uncomplicated grief, complicated grief, and disenfranchised grief.6 Anticipatory grief occurs before a loss when bad news is given or a loss is expected. Nurses can experience anticipatory grief when they see signs of poor prognosis or death. Uncomplicated grief is considered a ‘normal’ process and usually ends in acceptance of the loss.6 Complicated grief can be triggered by a traumatic loss, multiple losses, compounded grief, concurrent stress, or lack of support. Disenfranchised grief, which occurs in healthcare providers, can result when a loss is not openly acknowledged, socially sanctioned or publicly shared.5,6
Disenfranchised grief occurs with perinatal loss due to the death occurring before birth or shortly after, with society dismissing the loss quickly.4 There is no tangible evidence of the baby’s existence and few memories for people to share.7 When a nurse develops disenfranchised grief, the emotional and psychological aspect of life is disrupted. A sense of meaninglessness and feelings of injustice and inequity are felt.5 As nurses experience cumulative patient losses over time, they have compounded grief, which can result in trauma and increased anxiety.7
Perinatal nurse experiences
The birth of a child is considered a joyous occasion and a time to celebrate; it is a heartbreaking event to lose an infant or mother. Unfortunately perinatal loss and maternal death do occur, which results in grief not only for the mother and/or family, but also for the healthcare team. There are many different ways that staff cope with their grief over the death of a patient. Some may, for example, go to a bar after their shift to numb their feelings about the experience. Others may try to avoid caring for families that are experiencing an infant death. Some staff want to discuss the situation and their feelings with co-workers; others refuse to talk. They may maintain a stoic attitude and report not being affected by the death, while continuing to care for patients.
On one observed occasion, a nurse attending deliveries in a hospital was present at a fetal demise; afterwards, the nurse took the infant into a breakroom and sobbed while rocking the baby. The physician and other nurses were surprised at this reaction; they had to take the baby from the nurse so that the family could have time to say goodbye. The nurse was unable to appropriately care for patients during the remainder of the shift and had to take additional time away from work to resolve feelings relating to losing the infant.
Nursing care of critically ill or dying infants causes profound emotional stress that builds up over time.2 The unresolved grief places the nurse at high risk for compassion fatigue – the loss of ability to nurture – especially since there is little to no formal support to counteract the negative emotions involved in their role.8 Further, cumulative experiences of exposure to perinatal death can cause anxiety and trauma for nurses, rendering them psychologically unable to support babies and their families.9
Evidence of the problem
Initial symptoms of unresolved grief include anger, anxiety, apathy, depression, fatigue, guilt, headaches, helplessness, nausea and stress.10 If left unresolved or unrecognised, this may lead to chronic compounded grief, burnout (dissatisfaction with work associated with feelings of powerlessness that gradually progress),11 compassion fatigue, decreased productivity, high staff turnover and increased absenteeism, which, in turn can lead to staff departing the nursing specialty (Table 1)10 Furthermore, neonatal nurses are prone to the distress caused by grief because their training is geared towards rescue; therefore, the death of a patient may be viewed as a failure.9
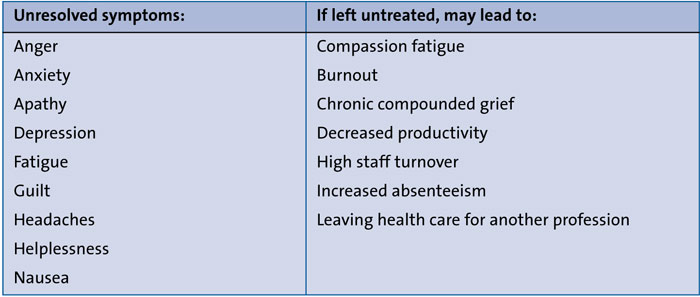
TABLE 1 Symptoms of stress and grief and the consequences.
Coping in other discipline areas
There is little information regarding safe, healthy ways for perinatal nurses to resolve and cope with grief encountered in the workplace. However, there is a plethora of evidence regarding oncology, hospice, and palliative care nurses coping with patient death. Oncology nurses have identified several ways to protect themselves when caring for patients that die. Some may alienate their friends and family outside of work by not sharing stories from their workplace.12 In this way, the nurse can feel that they are protecting their families; however, this may push the family away and reduce much needed support.12 According to research,12 other nurses may protect themselves from grief through their actions. Engaging in care activities helps the nurse feel that everything has been done to help the patient and family.
Some formal ways in which oncology and hospice nurses have been supported include:13
- peer support groups
- debriefing sessions
- counselling
- tranquility rooms
- massage chairs
- aromatherapy.
Other strategies have included encouragement of time to oneself and family, and time away from work to mourn.14
Maintaining control over emotions is a skill many nurses have mastered; they continue to care for patients and families without acknowledging their feelings, pushing aside their grief. However, multiple losses that are pushed aside and not processed can affect a nurse’s ability to provide effective care to patients and bitterness, yearning, emptiness, and numbness can develop in the presence of persistent grief.15
Support systems
Peer support appears to have the most significant impact on nurses’ handling of grief. Support from the management team is vital; providing grief resolution is essential.16 Nurses need to be supported by co-workers, the management and formal counselling or debriefing to facilitate grief resolution.10 By encouraging grief resolution, compassion fatigue and burnout rates decrease and the workforce will remain strong.10
There appear to be few formal support systems available for perinatal nurses. Evidence indicates that the number of nursing staff who feel supported, have formal support offered, or engage in counselling or peer groups is surprisingly low. In a study of 100 participants, 60% were not offered support, 87% did not receive information to seek support, and 65% did not know of potential resources to gain support after the death of a patient.17
Studies show that neonatal nurses possess inefficient grief management skills,9 yet hospitals and schools of nursing provide little education to prepare perinatal nurses for engaging in bereavement care. In order to engage in bereavement care, nurses must first acknowledge the loss and accept that death in perinatal care does occur.18 A nurse is expected to remain strong, set aside feelings and perform the job by caring for other patients and their families. Most nurses are very good at caring for others, but far less good at caring for themselves or for each other. Prioritising their own health and supporting colleagues is vital.
Enhancing knowledge and skills
Many nurses have not had sufficient or appropriate training to offer grieving families the support they need. Staff need to feel confident in their ability to provide the best care they can, and good training enables staff to learn from the experiences of others. A clear understanding of the importance of setting boundaries in caring relationships will help to mitigate stress and grief if/when it occurs. Nurse educators are in an ideal position to help nurses learn more about stress management and coping with grief through grief literacy training to acquire communication skills to interact with patients and their loved ones.15 Managing personal wellbeing
Building and maintaining personal resilience and wellbeing while working in the face of loss, death and grief is important. Healthy coping strategies and stress-relieving mechanisms will help. Taking time to work through emotions can be beneficial. Some self-care methods include:11,19
- accept that this intense work with traumatised families will have an impact
- learn about the psychological and physical signs of grief and burnout and stay alert for them
- be kind to yourself – take breaks, lunch, annual leave and balance work life with other activities and interests
- maintain a healthy lifestyle with balanced meals, sleep and exercise
- nurture supportive social relationships by connecting with friends and family
- develop a professional support network – attend debriefing sessions, reflective practice, etc
- attend counselling
- engage in community activities
- take time to laugh and have fun
- seek inner tranquility using nature to heal, eg walking outside, gardening, etc
- engage in meditative exercises, seek spiritual renewal
- develop hobbies and creative projects.
Sharing feelings and experiences
It is important for nurses to recognise that the need for support is not a sign of professional inadequacy or personal weakness and that they are probably not the only person affected in this way. When facing a perinatal loss, working as a team and offering each other support and understanding is vital. Many will find that sharing feelings and discussing experiences will be of benefit. Seeking out and utilising support can relieve grief and talking to co-workers can help to reduce some of the burden of grief.18
Group debriefing sessions
Strategies to address the impact of stress and grief at the level of the organisation will help to build and maintain resilience. The management can create a positive and supportive work environment, acknowledging and accepting that staff will experience grief.10 Perinatal nurses should be encouraged to attend formal support after a loss event, such as a group debriefing session or peer support group (FIGURE 1). The sessions promote emotional support for staff members, giving them a safe place to verbally express their feelings and listen to the thoughts of others who have been in the same situation.19,20 The formal support sessions can be helpful, informative and meaningful for those that participate.21 These sessions should take place within the week of the event to quickly provide an immediate review of the event.22 Everyone involved in the event should be invited to participate. The debriefing sessions should be conducted by someone trained in debriefing high-stress situations. Managers or hospital chaplains would be able to facilitate these sessions. Helpful strategies cited in debriefing studies include peer-supported storytelling and sharing.10 It is said that grief loses some of its sting and hope rises when suffering is voiced and brought into the open, helping the sufferer to feel supported and cared for.23
Strategies for grief resolution should be emphasised during the debriefing sessions. If a nurse desires one-on-one counselling, the debriefing coordinator should make recommendations to facilitate this.

FIGURE 1 A debriefing event. The debrief needs to be held in a private space where all involved feel safe to speak openly and honestly. Credit: Shore H, 2014.20
Outcome influences
Several factors may influence nurse participation in a debriefing session following a loss. The individual nurse’s beliefs about death may hinder or help in coping with stress and grief. Workload plays a large part in participation, as well as the availability of other nurses to cover the unit. If the nurse is working back-to-back shifts, they might be unwilling to participate in grief recovery classes because these take time away from relaxation and family time. Others may not want to talk about grief regarding perinatal death. Individual needs must be considered. An open-door policy should be employed to encourage participation in debriefing sessions. Additionally, hospital leaders must change the culture to make debriefing the norm following a perinatal loss.
Support from the management team
The involvement of the hospital management team could make a huge difference to the culture of staff wellbeing. Particular emphasis should be placed on supporting each other and supportive management (TABLE 2).24-28
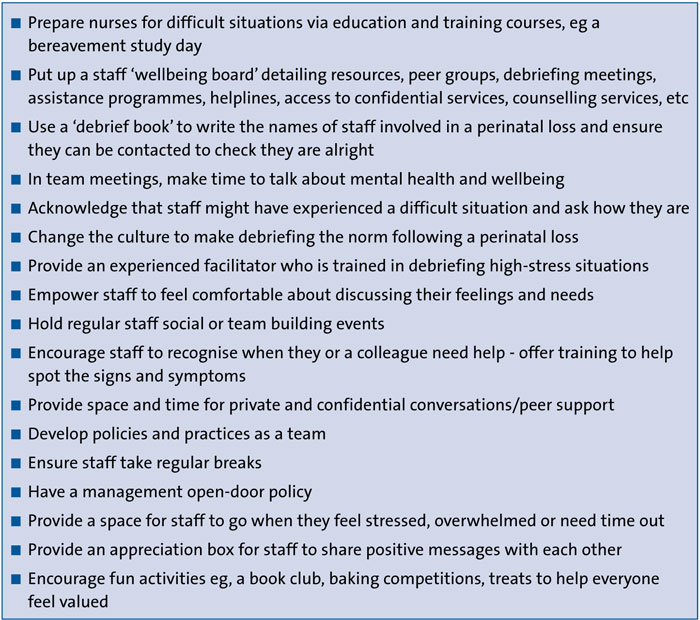
TABLE 2 Supportive management: practical advice for team managers.
Conclusion
Perinatal nurses are often involved in critical, end-of-life care situations leading to distress, grief, compassion fatigue, burnout and potential for a reduction in the quality of nursing care. There is a need for developing individualised coping strategies to resolve grief, and to ensure ongoing support for all staff involved in these emotional circumstances. Staff and the management team can help each other to cope with the stress and grief of patient loss. Together, nurses and management can develop new ways to support each other, enhance mental health and decrease burnout.
Author contributions
Dr Pankonien contributed the idea, background, and writing of the article.
Dr Groth contributed to writing, editing and formatting of TABLE 1.
Or read this article in our
Tablet/iPad edition
- Grief is a normal part of working with patients and their families.
- Developing coping strategies to resolve grief and supporting each other can decrease compassion fatigue and burnout as well as help to provide excellent nursing care.
- Nurses need to be cared for and supported if they are to carry on caring and supporting patients and their families.
Also published in Infant:
