

A midwifery-led newborn discharge pathway: an effective and innovative way of workforce management
Midwifery-led newborn discharge (MLND) is an effective way of reducing the length of hospital stay for well babies on IV antibiotics for suspected infection. A comprehensive protocol for MLND was designed and implemented on the postnatal ward following midwifery training in newborn discharge. Data were collected on the timings of chasing blood cultures and discharge from the time of starting antibiotics. The MLND pathway reduced the length of stay on the postnatal ward by 18.5 hours.
Anoop Pahuja
Neonatal Consultant
Garima Mishra
Neonatal Registrar
Luke Mills
Neonatal Consultant
Walton D’costa
Neonatal Consultant
Dilpreet Kaur
Paediatric Consultant
Chelsea and Westminster NHS Foundation Trust
Background
Workforce challenges in the NHS present a threat to delivering high-quality health services. Effective bed management can help maintain patient flow by efficiently utilising limited hospital resources, thus helping to provide high-quality care and improve patient satisfaction. Impaired patient flow leading to delayed discharge is a daily challenge and consumes an immense amount of time and energy from busy healthcare professionals. It can impede the quality of care and lower patient satisfaction.1
With limited resources, time constraints and the possible impact of Brexit and the global pandemic delaying recruitment of overseas doctors, there is no easy solution to the workforce problem. However, innovative ways of using the current workforce more efficiently by empowering and enhancing skills may help to achieve our goal of providing high-quality care.
As a busy level 3 neonatal unit in London, we are no different from other neonatal units in our struggle to recruit junior doctors. We recorded an increase in incidents of unnecessary delay in discharging mothers and babies. There are potentially many reasons for this but the most prominent reasons were delays in chasing blood test results and neonatal reviews due to staffing issues. This was hampering patient flow, distracting the medical team from delivering care and contributing to a poor experience for mothers, as reflected in our ‘friends and family’ feedback calling for an improved discharge process.
The Department of Health (2010)2 supports nurse-led discharge to improve patient flow and efficient use of beds in the NHS. It recommends that the plan must be agreed upon by the consultant in charge and the nurses have sufficient knowledge and expertise to execute the plan. This should not be overwhelming for nurses and the emphasis should be on a simple uncomplicated caseload and a supportive team.
A simple discharge can be defined as the discharge of a patient to their own home without complicated ongoing care needs that require complex planning (Department of Health, 2004).3 Nurse-led discharges are a well-established pathway in adult medicine such as surgery, obstetrics, medicine and a few paediatric sub-specialties, however, we could not find any reports or studies in neonatal medicine.4-6
We introduced MLND to overcome our workforce challenges and subsequently reduced the length of stay on the postnatal ward.
Methodology and design
The purpose of this article is to demonstrate the feasibility of MLND in effectively reducing the length of stay on the postnatal ward.
This was a prospective review of the length of stay of neonates on antibiotics for suspected sepsis on the postnatal ward over a period of three months between 1 July 2019 and 30 September 2019 after introducing the MLND pathway. The results were compared with the length of stay in a similar cohort before MLND was introduced over a three-month period between 1 April 2019 and 30 June 2019.
The midwives were actively involved in designing the MLND pathway. A clear and comprehensive MLND protocol was discussed and agreed at the clinical governance meeting. The protocol for newborn care was devised so that it would empower the midwives to provide care to the mother and baby as a single unit. Following appropriate midwife training on newborn discharge, low-risk babies would transfer to midwifery care. If a baby satisfied the criteria for the MLND pathway, it would be observed and monitored by the midwifery team. If all newborn early warning trigger and track (NEWTT) chart observations and C-reactive protein (CRP) levels remained normal with negative blood cultures, the midwives trained in the MLND pathway would discharge the baby home with no further review from the neonatal team. Both teams agreed to complete the MLND pathway form (FIGURE 1) and safely secure it in the medical notes. Special attention was given to ensure the safety of the newborn babies and to support the midwives. Regular and frequent training sessions were carried out to ensure the midwives were confident and competent in completing the NEWTT chart and MLND pathway and to maintain that at least 85% of midwives were trained on any given shift.
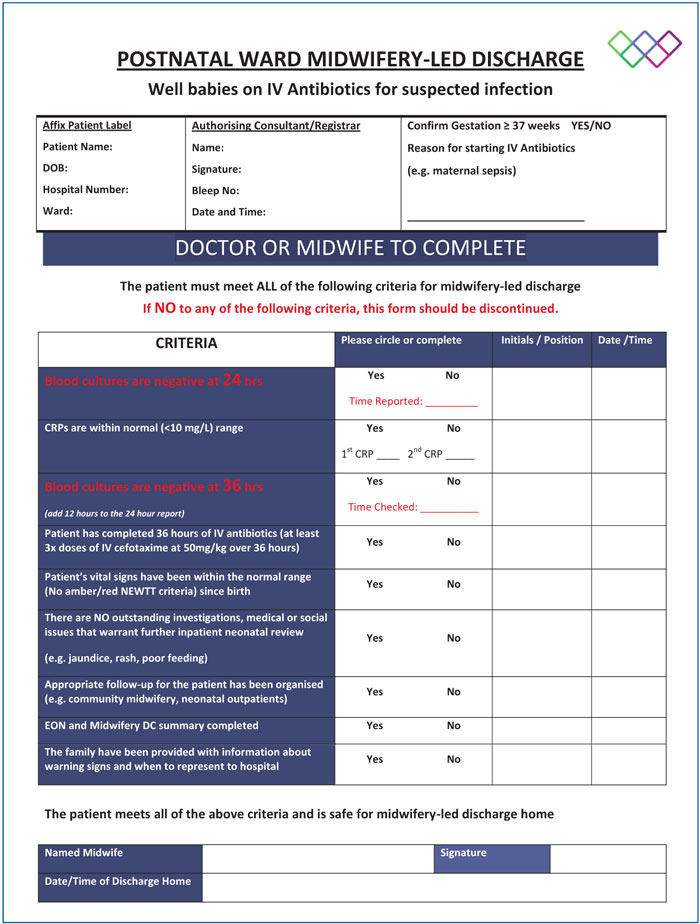
FIGURE 1 The proforma for the MLND pathway for well babies on IV antibiotics for suspected infection.
The MLND protocol was implemented following midwifery training in newborn discharge. Only ‘low-risk’ newborn babies on antibiotics for suspected sepsis qualified for inclusion on the MLND pathway. A low-risk newborn was defined as a newborn baby with suspected sepsis with normal observations on the NEWTT in the first 24 hours and normal CRP levels. Babies with abnormal NEWTT observations, abnormal blood results or other associated problems, or multi-system issues were excluded from the MLND pathway. Any newborn babies who stayed on the postnatal ward because of maternal reasons were also excluded. The decision to initiate an MLND protocol could only be made following discussion with the consultant in charge to ensure that only low-risk newborns were recruited onto the pathway.
If a baby met the criteria for the MLND pathway, a proforma (FIGURE 1) was filled in by the neonatal team after collecting blood for investigations for the septic screen. The midwifery team was trained to monitor the baby, record the observations on the NEWTT chart, chase CRP and blood cultures at 36 hours and enter all results on the MLND chart. If any concerns were recorded on the MLND proforma, such as abnormal observations on NEWTT and/or abnormal CRP or blood culture tests, the baby was excluded from the MLND pathway and instead, reviewed by the neonatal team until discharge.
Data collection
Implementation of the protocol was audited prospectively over three months. Data were collected from electronic patient records on:
- Indication of starting antibiotics.
- Time of chasing the blood culture tests.
- Time of discharge.
- Discharge process time (time from chasing the culture results to discharge). This is to include human factors, eg time required to prepare discharge documents, arranging discharge medications from pharmacy, etc.
As per our trust protocol, blood culture results are made available at 36 hours.7 If the culture result is negative, antibiotics are stopped and the midwives initiate the discharge process. Three hours were added to the blood culture report time to allow for administration time/human factors for arranging the discharge medication and preparing the discharge paperwork for the mother and baby. Every hour after the acceptable length of stay (ie 39 hours), was counted as an inappropriate delay in discharge.
Results
In the pre-MLND three-month period, 80 patients were selected as controls who would have met the criteria for MLND (TABLE 1). In the three-month period following implementation of MLND, 96 suitable babies were identified. Of these:
- 82 babies completed the protocol and were discharged by the midwives (TABLE 1)
- six babies were reverted to neonatal care for abnormal observations or abnormal blood results
- eight babies were excluded due to an extended stay for maternal reasons.
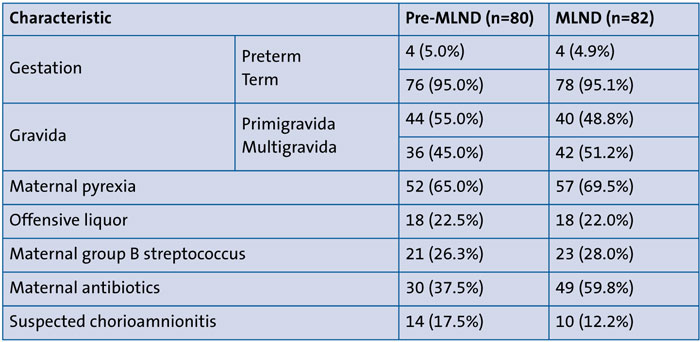
TABLE 1 Baseline characteristics of the babies on antibiotics in the two cohorts. Cohort 1 = pre-MLND pathway (1 April 2019 and 30 June 2019). Cohort 2 = MLND pathway (1 July 2019 and 30 September 2019).
In the pre-MLND period, many discharges were delayed for various reasons, for example, a delay in chasing blood results, doctors being busy in other priority areas, limited staff availability due to weekend services, and delay in discharge paperwork. The median discharge time was 66.5 hours (range = 40 to 99 hours) from the time of admission (FIGURE 2).
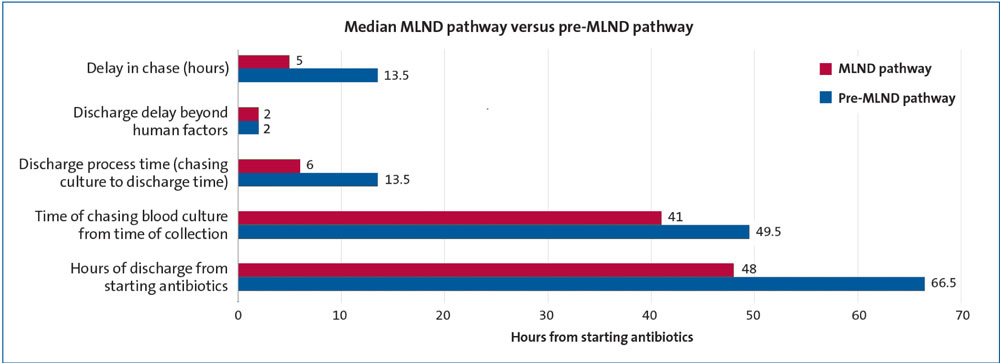
FIGURE 2 Before and after: improved patient flow on the postnatal ward following the introduction of the MLND pathway.
Following the introduction of the pathway, we noticed a gradual increase in MLND uptake with 22, 23 and 37 babies in July, August and September, respectively. The midwives appeared to gain confidence over the period and there was a reduced number of babies transferred back to neonatal care. This was consistent with an increased awareness of the pathway among the medical and midwifery teams. Regular support by senior midwives and a teaching programme provided by the midwifery development team helped to build the confidence of the midwives.
Over the three-month period, the MLND pathway improved patient flow on the postnatal ward by reducing delays in chasing blood cultures and discharge process times by half. Furthermore, the median time of discharge from starting antibiotics was significantly reduced to 48 hours (range = 38 to 60 hours). A few delays were noted over the weekend owing to limited staffing and reduced administrative support for the midwives and pharmacy staff, however, overall, we feel it was an impressive achievement to have reduced the length of stay by 18.5 hours (FIGURE 2). We intend to continue with the project aiming to improve on reducing the length of stay by using a multidisciplinary team approach involving the pharmacy and administration (to facilitate discharges), and extending the MLND pathway.
Discussion
The global pandemic and Brexit have exacerbated already existing workforce challenges within the NHS. The unavailability of medical personnel has led to delays in reviews and decision making thereby leading to delayed discharge, inefficient bed management and impaired patient flow – a daily challenge impeding quality of care and patient satisfaction.1
Midwives are the best support system for the mother-baby dyad on the postnatal ward, providing them with the necessary care to enable a smooth transition for discharge home. Midwives are trained to provide care for newborn babies including identifying early cues of any illness and recording necessary observations on the NEWTT chart. They are, therefore, the ideal candidates to look after low-risk newborns on antibiotics for suspected sepsis, once given the necessary training and with support throughout the process.
The MLND pathway has empowered our midwives to confidently manage and plan discharges for mother and baby; it has given them the independence and flexibility to plan discharges, reduce the length of stay and address issues of ward capacity and patient flow.
Before implementing the MLND protocol there were delays in discharges and these delays led to parent dissatisfaction in the postnatal wards, as reflected in feed-back and incident reporting. MLND has reduced the demand on the limited numbers of junior neonatal doctors on the postnatal ward, thereby enabling them to effectively use their time for training opportunities and management of babies in intensive care.
Without going into complex cost-effectiveness calculations, which is beyond the scope of this report, it is not difficult to envisage the positive impact on the finances of the postnatal ward by improving patient flow, reducing length of stay and avoiding costs associated with patient complaints following delays.
Often cost-effectiveness has a seesaw relationship with patient safety and it is crucial to find the right balance. Maintaining patient safety must be the key priority when adopting a new system of working. Our robust protocol provides a safe system with multiple checkpoints that ensures midwives feel confident in making safe decisions and only discharge babies after all criteria are met on the proforma. As highlighted by Fessey,8 regular teaching, training and assessment are the backbone of establishing a successful MLND system. Regular support from the neonatal team ensures it continues to be safe with no compromise to neonatal and maternal care. The midwives are autonomous bodies once the baby is transferred to their care although ‘round the clock’ medical team back up is in place, if required.
In this study, no complaints were received from patients with regards to MLND; the pathway was well supported. We collected feedback from parents and surveyed the midwives. 90% of the midwives were aware of and trained in completing the NEWTT chart and the MLND proforma. 85% felt that it improved patient experience and reduced length of stay, which is reflected in the study. They reported that they felt empowered and valued mother-baby dyad care. We received positive responses on the friends and family survey, especially for planning timely reviews and organising timely discharge. If parents expressed concern, the midwives were able to answer their queries and/or arrange medical review, though this was not required in the study period.
We will be aiming to formally assess patient satisfaction by incorporating an assessment of the parent perspective into the next round of audit.
Formalised MLND following an agreed protocol is a viable, safe way of improving the efficiency of discharge for low-risk neonates on routine postnatal care. We are sharing our MLND proforma here (FIGURE 1) should other units wish to adopt this model for reducing length of stay. However, further research is required to explore the full potential of MLND on the postnatal ward for other low-risk neonatal scenarios, eg hyperbilirubinaemia or hypoglycaemia.
Conclusion
Midwives are a vital support system for the mother-baby dyad on the postnatal ward, providing the necessary care to enable a smooth transition for discharge home. Use of a formalised MLND protocol is a viable and safe way to efficiently discharge low-risk neonates. By introducing the MLND pathway we have demonstrated efficient utilisation of resources to improve patient flow and reduce the length of stay on the postnatal ward by 18.5 hours.
Acknowledgement
With special thanks to the excellent midwifery team for their active involvement and support.
Or read this article in our
Tablet/iPad edition
- A midwifery-led discharge pathway is an innovative approach to improving patient flow and reducing the length of neonatal stay.
- A comprehensive protocol for midwifery-led care of well babies on IV antibiotics for suspected infection is presented. This will enable other units to develop their MLND pathway.
Also published in Infant:
