

Family integrated care – what, why and how?
Introducing the BAPM framework for practice
Nicola Crowley
Neonatal ST8 Grid Trainee, London, Darzi Fellow,Trainee representative member of the BAPM FICare working group
nicola.crowley@nhs.net
Nadia Leake
PhD Student, Newcastle University
Parent representative
member of the BAPM FICare
working group
n.leake2@newcastle.ac.uk
Aniko Deierl
Consultant Neonatologist, Imperial College Healthcare NHS Trust
Member of the BAPM FICare working group
Member of the FICare International Steering Committee
aniko.deierl@nhs.net
On behalf of the BAPM FICare working group
Background to the framework
The British Association of Perinatal Medicine (BAPM) had previously included family integrated care (FICare) into its clinical strategy and as a result of this, Family Integrated Care – A Framework for Practice,1 was published on 17th November 2021 helping neonatal units to work towards implementing this care model. The working party consisted of doctors, nurses, a parent representative, network leaders and representatives from Bliss. The framework is essential reading for all healthcare professionals working in a neonatal environment.
Family Integrated Care –A Framework for Practice.
The framework seeks to support the implementation of a model and philosophy of care within which families are enabled to be primary caregivers to their babies in partnership with the clinical teams. It acknowledges that many units will have already embraced some or all elements of the founding principles of FICare however, it stresses the importance of the cultural change that needs to occur so that parents are treated as equal, respected and essential members of the team caring for and participating in shared decision making about their baby. It also highlights the importance of a standardised and consistent approach to FICare as babies move between levels of care within a unit and to other units in the network, acknowledging that the approach may look slightly different in different units.
The framework includes key components to network approaches to implementing FICare. It has an extensive appendix that includes the summary of evidence for FICare, a list of useful resources and few examples of pioneering good practice.
What is family integrated care?
FICare is a model and philosophy of neonatal care, which promotes equal partnership between families and staff when caring for their baby/babies on neonatal units. FICare aims to build on the principle of family centred care, ultimately aiming to encourage and support parents to become their baby’s primary caregiver and share the decisions about their baby’s care. Becoming the ‘primary caregiver’ means the parents/carer are enabled and empowered to carry out the majority of their baby’s care confidently and independently once they have received adequate training and coaching.
There is conclusive and growing evidence that FICare produces clinical benefits for babies,2-6 improves mental health and reduces anxiety for parents2,3 during and after their stay on a neonatal unit3 and benefits staff too.7
As well as these cited benefits, as part of the NHS five-year plan, the Neonatal Critical Care Transformation Review has specified that parents should be more actively involved in their baby’s care and implementing FICare achieves this.8 Units working towards their UNICEF Baby Friendly accreditation will also have to show evidence of working in partnership with parents.9
The five key principles of FICare
The UK framework describes five key principles of FICare (FIGURE 1), which differs from the four original Canadian pillars of FICare previously described by O’Brien.2 FICare has since evolved in different countries and care settings and, over time, there has been increasing recognition that partnership with families is one of the most challenging culture changes to achieve and embed in practice. The working group, therefore, felt it was essential to include partnership with families as the fifth principle as everything should centre around this (FIGURE 2).

FIGURE 1 The five key principles of FICare.
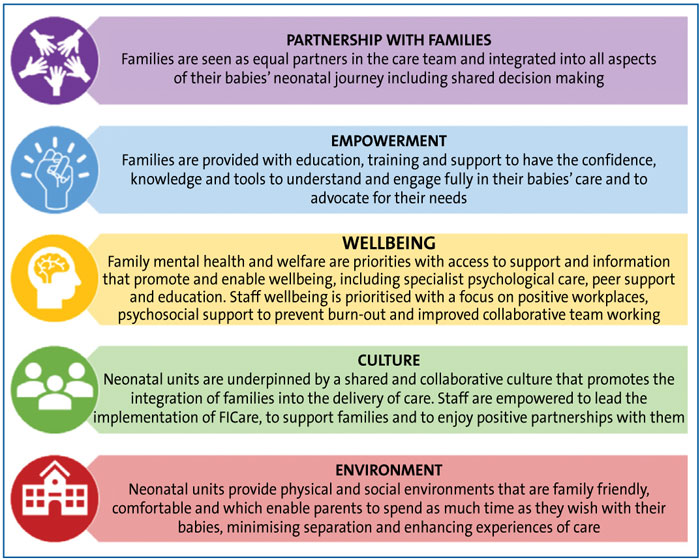
FIGURE 2 Short definitions of the key principles of FICare.
FICare is important – the parents’ perspective
The capacity of parents to form enduring bonds with their infant is one of the fundamental features of human experience. Bonding is considered the central developmental force across the lifespan.10 When we consider this statement, it is little wonder that admission to the neonatal unit – a sudden and prolonged separation soon after birth – leaves such an indelible mark on the psyche of parents and is considered a contributing factor in the persistent incidence of behavioural and learning problems among preterm infants.11 The FICare model ensures that parents can minimise disruption to bonding and create space for the necessary care and love that only parents can provide for their baby. FICare promotes skin-to-skin contact creating a protective environment for the baby, and brings the family experience as close to normality as possible, bridging the gap between a traumatic life changing experience and what families dream of when their baby is born.
While it is heartwarming to describe all the benefits of FICare, its importance can only be fully appreciated when we consider the trauma that can occur in its absence. The Bliss mental health survey of 589 parents in 2018,12 revealed that 80% of parents whose babies were admitted into neonatal care thought that their mental health suffered after their experience. 16% of parents surveyed were diagnosed with post-traumatic stress disorder after their time on the neonatal unit, and 39% of parents felt they had developed a mental health condition after their experience on the unit, although not officially diagnosed.
From the parents’ perspective, having experienced neonatal intensive care admissions to units with and without a culture of FICare, we understand that every day on a neonatal unit without FICare is an opportunity for trauma to occur. Parents report
that FICare can restore their parenthood, give them family time, and support better mental health and the neurological development of their child.
These two elements are intertwined; the health of the parent-baby unit is interdependent. FICare acknowledges that the implementation of the framework ensures that families are protected from this trauma as much as possible.
The role of parents when FICare is the standard model of care
When FICare becomes the standard model of care:
- parents are integrated partners in care
- parents are primary caregivers and involved in care as much as possible
- parents are informed and understand all aspects of care
- parents are involved in the decision-making process on a daily basis
- parents coproduce (parents and staff) and regularly evaluate the FICare programme delivered locally, which is iterated accordingly.
Tips to help implement FICare on your unit
- Get support from all senior leaders (nursing and medical). The unit needs to ensure FICare implementation is a unit priority and include it in the clinical strategy accordingly. Acknowledge this is not a quick quality improvement project; this is a service improvement project that requires change in multiple domains, which will take time to introduce and implement. Decisions need to be made about which areas/change ideas to initially focus on.
- Find your core team/champions/advocates for families/drivers; ensure you have multidisciplinary team representation. With champions, identify the elements of family centred care and FICare already in place on your unit and use this scoping exercise to identify areas needing improvement. There is a self-assessment tool available to help with this.13
- Ask parents (current and past) from your unit what they feel they ‘need’ or could have benefitted from. Ensure you build your FICare programme around these opinions.
- Don’t wait to implement FICare when the babies are nearing home. Establishing partnership with parents should start antenatally whenever possible, followed by the delivery experience in the same ethos and continued across all areas of the unit and network. Parents need staff to explain to them as soon as possible that their interaction and presence improves outcomes for their baby and also their own mental health.
- Staff must accept the culture of working in partnership. It cannot be an opt in or out way of practising for healthcare professionals; it needs to become the standard model of care practised on your unit.
- Ask non-champion staff what they are worried/fearful about regarding the introduction of FICare and identify any barriers.
- Coproduce the materials with parent and staff champions, and any other staff who are interested. However, don’t feel you need to reinvent the wheel; borrow, adapt and share with and from other units who are potentially more ahead on the FICare journey.
- Identify the times of the day when parents are most commonly on the neonatal unit and try and build flexible modes of training around these times.
- Train staff before launching as a FICare unit, ensuring they all understand why FICare is essential and addressing the fears they have previously expressed. The success of becoming a unit that practises FICare is based on the culture of the team. Ongoing regular training of staff will be needed, addressing new skills such as coaching, advanced communication and practising in a trauma-informed way.
- Regularly evaluate the resources and programme by asking staff and parents for their feedback and adjust accordingly.,
Funding and resources
The framework explains that, while the fundamental base of FICare can be implemented at low cost, it does stress that additional funding is needed to ensure successful and sustainable implementation. Units who have already been successful at implementing FICare have learnt the importance of dedicated staff/staff time available to:
- assist the team during the implementation phase
- provide and coordinate ongoing parent and staff education
- create and update resources
- improve the environment to provide the very best experience possible for families.
Conclusion
FICare is a holistic care model that has been proven to improve neonatal outcomes and parental mental health. The authors and the BAPM working group hope that Family Integrated Care – A Framework for Practice1 will be a useful document for UK neonatal units and provide a practical approach on how to work towards this care model.
Or read this article in our
Tablet/iPad edition
