

Designing a neonatal teaching programme that works for trainees
A high-quality and effective local neonatal teaching programme is essential for the education and development of paediatric trainees and the wider multidisciplinary team. Trainees themselves may be best placed to guide and develop educational provision, having the greatest insight into their educational requirements. We demonstrate the redesign of a multidisciplinary postgraduate teaching programme in a regional level 3 neonatal intensive care unit through an easily replicable quality improvement project.
Patrick Blundell
Senior Clinical Fellow and Neonatal
Chief Resident
patrick.blundell@wales.nhs.uk
Heidi Green
Advanced Neonatal Nurse Practitioner and
MDT Educational Governance Lead
Amar Asokkumar
Consultant Neonatologist and Neonatal Local Programme Director
Regional Neonatal Intensive Care Unit, University Hospital of Wales, Cardiff
Background
The Royal College of Paediatrics and Child Health (RCPCH) Trainee Charter states that trainees should be provided with ‘high-quality, relevant, varied teaching locally’,1 with this being essential for trainees to develop the clinical skills and knowledge required to meet curriculum requirements.2
To maintain high standards for educational provision, it is essential that training units continually evaluate and develop teaching programmes, centered on evolving educational needs and contemporary trainee feedback. It is argued that this process of educational governance is best led by trainees themselves, having the strongest insight into their own learning needs, and those of their peers. With this in mind, the role of ‘chief resident’ is emerging within training units in the UK, with these junior doctors ideally placed to evaluate and direct educational change.3 The COVID-19 pandemic had a drastic impact on postgraduate medical education locally and nationally,4 with the postponement of the majority of formal teaching. Furthermore, the conflict between service provision and medical education has only been exacerbated by the pandemic.5 Following a hiatus, there was an opportunity for a new education team to redesign the ageing local teaching programme, developing it with the multidisciplinary approach in which modern neonatal care is provided, making it work for trainees, and the training unit.
Aims
The aim of the project was to design and implement a new weekly multidisciplinary teaching timetable for commencement in September 2020. Improvements would be guided by trainee feedback. The new teaching programme would better reflect the RCPCH Progress curriculum,6 including the key domains of:
- communication
- procedures
- patient management
- leadership and team working
- patient safety including safe prescribing
- education and training
- research.
Setting
The project was undertaken within the regional neonatal intensive care unit at the University Hospital of Wales, Cardiff. The unit provides tertiary neonatal medical care alongside regional surgical and sub-specialty services, with a maximal operating capacity of 32 cots (12 intensive care, eight high dependency, 12 special care). Junior medical staffing includes eight tier 2 doctors, 12 tier 1 doctors, eight advanced neonatal nurse practitioners (ANNPs) and one physician associate.
Engaging stakeholders
A multidisciplinary education team was formed comprising the local programme director, an ANNP, neonatal staff nurses and a paediatric trainee acting as ‘chief resident’. The consultant body, paediatric trainees, clinical fellows and neonatal nurses were all engaged early, with widespread support for improving the teaching programme. The project also met health board level directives to improve patient safety through education and simulation involving scenarios identified by incident reporting and risk management.
The project
A Plan, Do, Study, Act (PDSA) cycle7 was used to undertake improvements. Trainee feedback was gathered through anonymous electronic forms. Previous timetabled teaching sessions (TABLE 1) were rated (1-10) on their educational merit, alongside free text responses. Nurses were asked for feedback on barriers to attendance. The new teaching timetable (TABLE 2) was constructed using feedback, underpinned by curriculum domains. Poorly rated sessions were removed. Consistent feedback suggested sessions should be more interactive and ‘shop floor’ based to help facilitate attendance, with more focus on simulation and practical procedures. Sessions were consultant, ANNP and trainee delivered, to allow demonstration and development of teaching skills. The majority of sessions were 30-45 minutes in duration to allow for the delivery of sufficient content while maintaining attention and educational benefit. Teaching was delivered ‘bleep free’ with the second on-call consultants holding the emergency bleep during sessions.
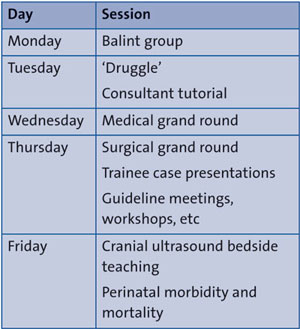
TABLE 1 The original weekly teaching timetable.
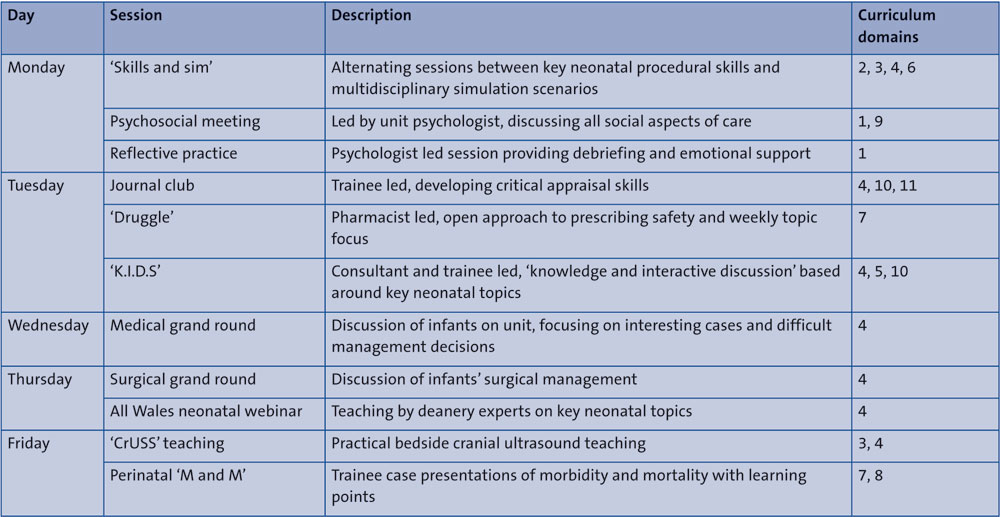
TABLE 2 The improved weekly teaching timetable with session descriptions and linked progress curriculum domains (1 = Professional values and behaviours and professional knowledge; 2 = Professional skills: communication; 3 = Professional skills: procedures; 4 = Professional skills: patient management; 5 = Health promotion and illness prevention; 6 = Leadership and team working; 7 = Patient safety including safe prescribing; 8 = Quality improvement; 9 = Safeguarding; 10 = Education and training; 11 = Research).
Following the first five months of implementation, feedback was gained to measure improvement and guide further development. Ratings for ‘overall educational value’, ‘quality of content’ and ‘quality of formats’ had all increased following the intervention (median score of 7/10 increasing to 8/10 for all domains). The new teaching formats gained positive feedback with median ratings consistently upwards of 9/10. Free text responses echoed positive session ratings. However, comments continued to describe the demands of service provision as barriers to medical and nursing attendance. Further feedback will be gained on a bi-annual basis to continue the PDSA cycle of improvement.
Learning and future steps
Having a structured, multidisciplinary approach to developing educational provision was key to implementing effective change. Putting trainees at the heart of educational governance through regular feedback and the ‘chief resident’ role helped to drive and focus improvement in areas of greatest need. Simple changes, for example standardising session start times, had large impacts on attendance and punctuality.
Having a rigid weekly timetable often disadvantaged less-than-full-time trainees with set ‘off days’, as the same sessions were frequently missed. Solutions to this issue will be explored in future cycles. Improvements are still required with regards to the balance between education and service provision. Nursing attendance at teaching improved somewhat but remained inconsistent. Further cultural change is required before teaching is regularly attended by all multidisciplinary team members, however this would undoubtably result in improved patient care.8,9
Acknowledgement
The authors would like the thank Dr Ian Morris (Consultant Neonatologist) for his enthusiasm and support with the project.
Or read this article in our
Tablet/iPad edition
- The RCPCH mandates that trainees are provided with ‘high-quality, relevant, varied teaching locally’.
- Trainees may be best placed to guide the development of teaching provision through contemporary feedback and local educational governance roles.
- Neonatal teaching may be better delivered in the multidisciplinary way in which neonatal care is provided.
Also published in Infant:
