

COVID-19: effects on breastfeeding rates at discharge from the NNU
The World Health Organization recommends exclusive breastfeeding for six months following the birth of an infant1 and exclusive breastfeeding on discharge from neonatal units (NNUs) in the UK is highly recommended. Despite this, mothers may face many barriers that make breastfeeding difficult including prenatal, medical, societal, hospital and sociocultural issues.
Lizaveta Collins1Paediatric Trainee ST6
lizaveta.collins@gmail.com Saadia Rao2
Paediatric Consultant Philip Adedokun2
Paediatric Trainee ST1 Jo-Anne Johnson3
Senior Lecturer 1Rosie Hospital, Cambridge University Hospitals NHS Foundation Trust
2Colchester General Hospital, East Suffolk and North Essex NHS Foundation Trust
3Anglia Ruskin University School of Medicine, Chelmsford
Infants who are admitted to a NNU are at risk of growth failure, developmental delays, necrotizing enterocolitis, broncho-pulmonary dysplasia and late-onset sepsis. Hence, mother’s milk should be their primary enteral diet. Yet infants admitted to a NNU are frequently unable to feed by breast or bottle because of ill health or prematurity. These infants require nutritional support until they can start oral feeding and the mothers need support from healthcare staff to build up an adequate long-term milk supply. A lack of support for new mothers in the critical period of the first few days can lead to potential breastfeeding problems and early weaning.
SARS-CoV-2 (COVID-19) was first reported at the end of 2019; the COVID-19 restrictions officially began in the UK on 23 March 2020. Since then, the healthcare system has come under considerable pressure with staff availability reduced. All UK hospitals introduced a COVID-19 policy that applies to visiting and many NNUs have a restriction where only one parent can visit a baby on the unit.
We aimed to assess if the COVID-19 lockdown impacted on a woman’s ability to breastfeed her infant in our level 2 NNU by looking at breastfeeding initiation and rates at discharge from the NNU.
Aims and methods
Colchester General Hospital has a level 2 NNU and the majority of babies who are admitted to the NNU are premature babies. The unit accepts premature babies born from 28 weeks’ gestation, however in exceptional circumstances, babies as young as 23 weeks’ gestation born at the hospital might be admitted and transferred to the tertiary centre within the first 24 hours of life. Term infants diagnosed with conditions such as respiratory distress, suspected sepsis, hypoglycaemia or hypoxic ischaemic encephalopathy may be admitted for a short stay.
This was a retrospective study. We used the BadgerNet neonatal system (the electronic national register of babies admitted to a NNU) and Evolve, a local data system at Colchester General Hospital. We looked at the first day where expressed breast milk (EBM) or breastfeeding was introduced and the number of babies breastfeeding at the time of discharge.
We reviewed breastfeeding trends over two periods:
- Period 1 – between 1 March 2019 and 1 December 2019 prior to the COVID-19 pandemic
- Period 2 – between 1 March 2020 and 1 December 2020, when the COVID-19 lockdown rules were implemented as per hospital policy and only one parent was able to visit the baby at the NNU.
At our hospital, all mothers are asked what their feeding preferences are on admission to the NNU. The importance of breastfeeding is explained to all mothers of premature and term infants. Where breastfeeding is not possible, the mother is advised to express milk until the baby is able to feed at the breast. Milk expression equipment is provided along with an educational session with the midwifery team.
Results
During period 1, there were 535 infants admitted to the NNU. Of these, breast milk/colostrum was introduced to 171 babies on day 1 (31.5%). There were 380 infants admitted to the NNU during period 2 and there were 91 babies (23.9%) that received breast milk/colostrum on day 1 (TABLE 1).
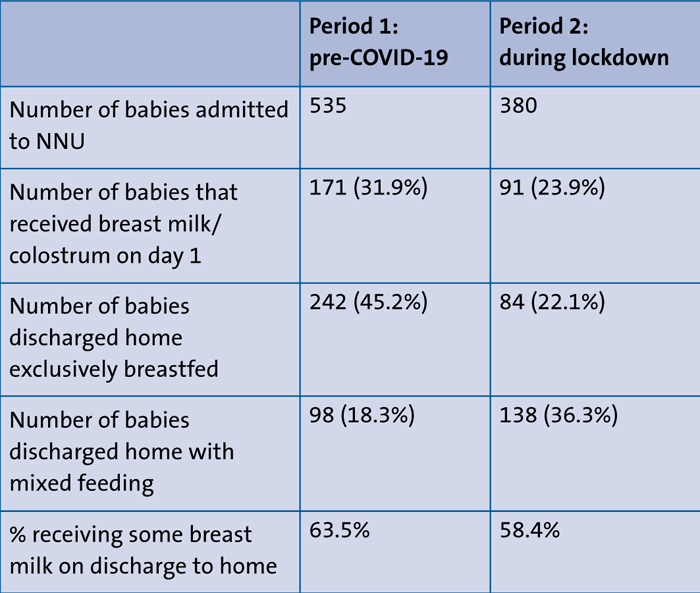
TABLE 1 Breastfeeding trends over the two time periods.
During period 1, we identified 242 (45.2%) babies that were discharged home exclusively breastfeeding. During period 2 the percentage of infants who were discharged home exclusively breastfeeding fell to just 84 (22.1%).
Before the COVID-19 lockdown, 98 babies (18.3%) were discharged to home mixed-feeding; 63.5% of infants were discharged home receiving some breast milk in Period 1.
During the COVID-19 lockdown, 138 babies were discharged home mixed-feeding; 58.4% were receiving some breast milk on discharge but the proportion of exclusively breast milk fed infants was much lower.
Discussion
From our data analysis it would appear that the COVID-19 restrictions in 2020 impacted breastfeeding rates in the NNU. However, this is a retrospective study that only considers two time periods and does not consider, for example, the level of support offered to women, the clinical condition of the babies, the length of stay and many other confounding factors.
During the pandemic, there are several potential factors that might disrupt breastfeeding prevalence, for example:
- limitations in the availability of skilled health workers and/or the provision of health services
- changes in clinical practice indirectly leading to disruption in breastfeeding prevalence
- lack of support for new mothers in the critical first few days
- reduced infant feeding support from fathers and other family members
- disruptions to the enabling environment
- reluctance by mothers to breastfeed because of perceived risk of COVID-19 transmission
- lower coverage of breastfeeding support services in antenatal care
- reduced skin-to-skin contact
- effects on maternal mental health
- less contact with other mums on the NNU therefore less sharing of experiences
- early discharge from neonatal services.
Since the start of the pandemic, the healthcare system has been under a lot of pressure and it is likely that support for new mothers from staff was reduced during 2020. Also, at the time, only one parent could visit the unit so it is likely that the mother felt isolated and did not have support to breastfeed from the staff or her own family. She might have been anxious travelling to the hospital and might have preferred to spend time just being with her baby, rather than breastfeeding or expressing milk.
We cannot be certain that the intention to breastfeed among our mothers was the same in both periods as it is possible that some mothers were reluctant to breastfeed because of perceived risk of COVID-19 transmission. However, oral feeding requires careful and intensive management, particularly in preterm infants and those with clinical needs. During the lockdown restrictions, mothers were less able to communicate with staff via the usual communication platforms, especially face-to-face, and this will have led to minimum support with breastfeeding during pregnancy and after birth, resulting in disrupted breastfeeding behaviours and a decrease in breastfeeding rates.
Rather disappointingly, we see from our analysis that the majority of infants admitted to the unit were not introduced to colostrum within the first 24 hours of age; this was across both observed periods meaning that we were not meeting expected standards pre-COVID. In addition, our exclusive breastfeeding rates at discharge pre-COVID were <50%. Our mothers are frequently encouraged to express breast milk by the nursing and medical staff; however, it would seem that there are a number of steps that healthcare professionals should take to protect and promote breastfeeding during COVID-19 and beyond:2
- support the mother to make informed decisions about feeding
- position the baby at the mother’s breast within the first hour of birth
- keep mother and baby together whenever possible
- ensure regular skin-to-skin contact
- give maximum support to mothers during the first few days of birth to help them to initiate and maintain an adequate milk supply
- initiate a milk supply with pumps where necessary
- many mothers stop breastfeeding because they feel that their milk supply is inadequate; reassure women who might feel this way and, where appropriate, encourage milk expression to build an adequate supply
- hospitals should develop adequate training for staff to deliver skilled breastfeeding counselling to mothers and families via online platforms
- at discharge, discuss with mothers the importance of regular, frequent breastfeeding
- encourage community-based lactation support (eg midwives, electronic communication platforms, breastfeeding cafes).
COVID-19 has had a significant impact on maternal and neonatal clinical practices3-7 and the healthcare community should come together to discuss how we can improve our services to protect breastfeeding. It is important to find innovative solutions to ensure that access to breastfeeding support services is not disrupted and that families – especially those with babies in the NNU – continue to receive breastfeeding counselling.
Or read this article in our
Tablet/iPad edition
