

Sodium valproate – can it mask neurohypophyseal diabetes insipidus?
Neonatal central diabetes insipidus (DI) is an uncommon disorder. It is characterised by polyuria, hypernatraemia, high plasma osmolality, and low urine osmolality. Sodium valproate is a drug used for seizure treatment; its use in adult patients to treat DI has been reported in the literature. We report a case of neonatal neurohypophyseal DI managed with sodium valproate for refractory seizures. Sodium valproate may have contributed to the improvement in DI symptoms by increasing the production of antidiuretic hormone. To our knowledge, no such association has been reported for neonatal DI.
Femi AdeniyiST6 Paediatrics
femi.adeniyi@nhs.net
Dennis Padi
ST5 Paediatrics
Sanjeev Rath
Neonatal Consultant
Sarah Thompson
Neonatal Consultant
Arrowe Park Hospital, Wirral University Teaching Hospital, Wirral
The case
Here, we report a case of transient neurohypophyseal DI in a late preterm female neonate. She was born at 35+4 weeks’ gestation to a 31-year-old multiparous woman who presented to the local hospital with severe antepartum haemorrhage. There were no pregnancy concerns – antenatal scans and screening serology were normal – and there were no maternal risk factors for sepsis. The background maternal history included polycystic ovarian syndrome and DI, which was treated with desmopressin, an analogue of the hormone vasopressin (also called arginine vasopressin, AVP, or antidiuretic hormone, ADH) from four years of age. There were no health concerns reported in any other siblings.
The infant was delivered by an emergency caesarean section in a district general hospital for suspected placental abruption. She needed extensive resuscitation with intubation, external cardiac massage, three doses of adrenaline, 0.9% saline bolus and an emergency packed red blood cell transfusion. Her heart rate was detected to be above 60 beats per minute at 16 minutes of life with her first gasp at 29 minutes. Her venous cord blood gas analysis showed:
- pH=6.8
- pCO2=12.1kPa
- base deficit= -21.7mmol/L
- lactate=15 mmol/L.
She was commenced on passive cooling and transferred to the neonatal unit at the district general hospital. At two hours of age, she had seizures and required treatment with loading doses of phenobarbital and midazolam followed by a midazolam maintenance infusion, as per the local guidelines, prior to being transferred to the tertiary neonatal unit.
At the neonatal intensive care unit (NICU), she continued to have refractory seizures. She received a further loading dose of phenobarbital and escalation of the midazolam infusion. The cerebral function monitoring (CFM) was abnormal, demonstrating a burst suppression pattern with frequent spikes consistent with episodes of seizures (FIGURE 1). Her seizures finally stopped with a loading dose of phenytoin.
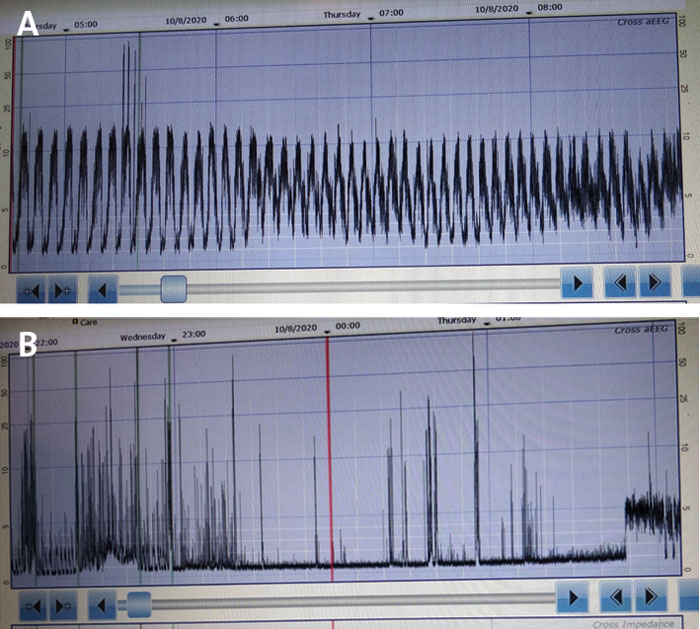
FIGURE 1 Cerebral function monitoring. A) Showing refractory seizures. B) Showing burst suppression.
Haematological and biochemical laboratory parameters revealed:
- deranged coagulation on admission (prothrombin time, PT=27secs; activated partial thromboplastin time, APTT=73secs; fibrinogen=0.6g/L; international normalised ratio, INR=2.4)
- thrombocytopenia (67 x 109/L)
- polycythaemia (haematocrit level=0.64)
- raised transaminase (aspartate aminotransferase test, AST=97 IU/L) and troponin (517ng/L).
She received fresh frozen plasma and was commenced on intravenous vitamin K. The thrombocytopenia, polycythaemia and deranged liver enzymes normalised over the course of her admission in the NICU. She was commenced on broad spectrum antibiotics following a septic screen at the district general hospital; antibiotics were discontinued at 36 hours once the blood culture results were negative. The UK newborn blood screen was reported as normal for sickle cell disease, cystic fibrosis, congenital hypothyroidism, phenylketonuria, medium chain acyl-Co A dehydrogenase deficiency, maple syrup disease, isovaleric acidaemia, glutaric aciduria type 1, and homocystinuria.
During the admission at the NICU, the infant continued to have subtle seizure clusters manifesting as cycling movements of the upper and lower limbs. Levetiracetam was added for the ongoing seizure clusters but was not effective. Following discussion with the neurologist, sodium valproate was commenced and this stopped the seizures. Once seizure control was established, the levetiracetam was gradually weaned. The liver function blood tests and full blood count remained within normal ranges while the infant was on sodium valproate. Neurological examination of the infant revealed generalised hypotonia, poor suck and swallow, and an absent gag reflex. She developed severe reflux and aspiration pneumonia at around 5-9 days of admission to the NICU. She was managed with hyoscine butylbromide for excessive pooling of secretions in her oropharyngeal cavity, and Gaviscon and omeprazole for gastro-oesophageal reflux. Her feeds were given via a nasogastric tube due to the risk of aspiration.
On day four of life, she was noted to have an elevated serum sodium level of 154mmol/L. She was fluid restricted as part of the management of hypoxic ischaemic encephalopathy (HIE) and the rise in serum sodium was considered secondary to dehydration. Following liberalisation of fluid volume, her serum sodium normalised to 145mmol/L within 24-48 hours, only to be elevated again to 156mmol/L on day 5 of life; at that point she was polyuric with a urine output of 6.7mL/kg/hour. Investigations showed serum osmolality of 309mOsmol/kg with paired urine osmolality of 145mOsmol/kg (TABLE 1).
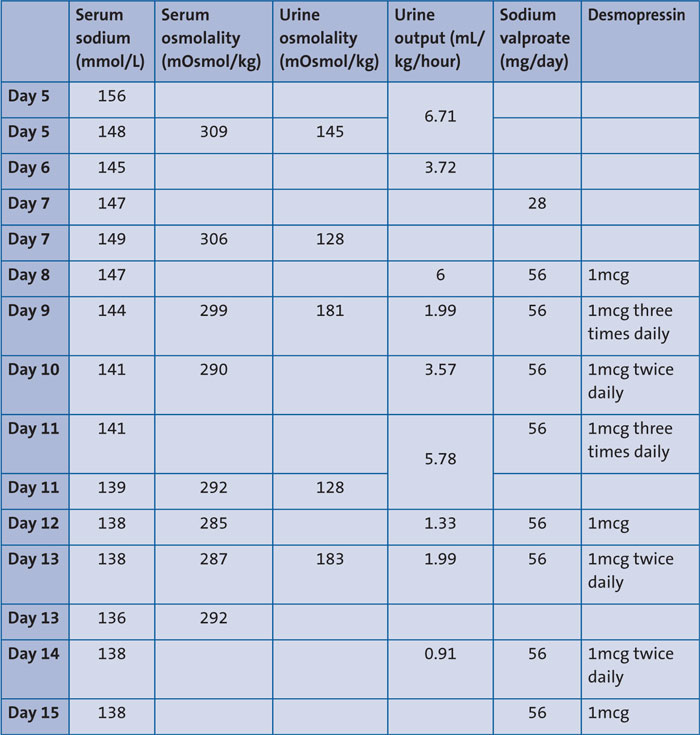
TABLE 1 A timeline of laboratory investigations and drug administration.
In view of the high serum sodium (156mmol/L), high serum osmolality (309mOsmol/kg) and low urine osmolality (145mOsmol/kg), a diagnosis of DI secondary to HIE was considered. The case was discussed with the tertiary endocrine team who agreed with the possible diagnosis and advised commencing desmopressin. The infant’s serum sodium, urine output, serum osmolality and urine osmolality subsequently normalised and desmopressin was discontinued on day 15 of life at the local hospital. We noted that sodium valproate as a seizure medication was commenced at the same time as the desmopressin.
Head magnetic resonance imaging (MRI) showed a structurally normal brain with normal cerebellum, corpus callosum and pituitary gland. The thalami appeared to ‘signal’ with a higher intensity than normal. On diffusion weighted images, there were extensive areas of restricted diffusion present within the basal ganglia, lentiform nuclei and thalami with abnormal diffusion within the corpus callosum (FIGURE 2).
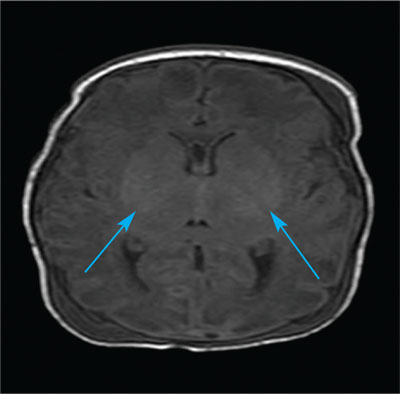
FIGURE 2 Head MRI showing extensive areas of restricted diffusion present within the basal ganglia, lentiform nuclei and thalami with abnormal diffusion within the corpus callosum.
The infant remained in the NICU and received ventilation for six days and non-invasive ventilation (continuous positive airway pressure) for four days before being finally discharged to the local hospital on low-flow oxygen on day 14 of life.
Discussion
Neonatal central DI is an uncommon disorder which is characterised by polyuria, hypernatraemia, high plasma osmolality, and low urine osmolality. Aetiologies discussed in the literature include central nervous system malformations, intracranial haemorrhage, intracranial infections, trauma, inflammation, HIE, and inherited mutations in coding for AVP in familial neurohypophyseal DI.1
This case presented a dilemma to the team regarding the aetiology of DI: it could be DI secondary to HIE or familial DI, as the mother had been diagnosed with DI at four years of age.
Familial neurohypophyseal DI is a rare inherited disorder with the majority inherited in an autosomal dominant pattern. A mutation in the 2.5kb AVP-neurophysin II (AVP-NPII) gene located on chromosome location 20p13 results in a deficiency of AVP.2,3
Neonatal central DI has been linked to various aetiologies, such as congenital infections, neonatal stroke/haemorrhage, HIE, and cerebral abscess.4,5 In our index case, the diagnosis of central DI secondary to HIE was made due to the perinatal events (severe antepartum haemorrhage in the mother, poor condition at birth needing extensive resuscitation) and the further clinical course and investigations suggesting multi-organ involvement.
MRI showed changes in the basal ganglia, in keeping with HIE. The presence of normal thyroid stimulating hormone (TSH), blood glucose and cortisol (glucose=3.5mmol/L; TSH=5.64mU/L; thyroxine, T4=21.7pmol/L; cortisol=357nmol/L) and absence of other pituitary hormone levels for comment, made the diagnosis of neurohypophyseal DI secondary to HIE a likely possibility, rather than a confirmed aetiology.
Most case reports of neurohypophyseal DI have shown an abnormal pituitary gland on MRI and abnormal hypothalamic pituitary function. However, there is a case report describing similar findings to our case, ie normal pituitary gland on imaging and normal hypothalamic-pituitary axis function.6,7
The anticonvulsive medication sodium valproate has been linked to causing hyponatraemia, attributed to increased ADH production in an adult case report.8 It is worth mentioning that our case was commenced on sodium valproate due to recurrent seizures, despite the use of levetiracetam. It was noted that the weaning of desmopressin since the commencement of sodium valproate was rapid. The raises the possibility that sodium valproate used in the index case could have stimulated the production of ADH. There have also been reports of hyponatraemia and/or syndrome of inappropriate secretion of ADH (SIADH) in association with sodium valproate.9-11
The index case continues to be on sodium valproate and remains off desmopressin with no symptoms of DI. Once sodium valproate is stopped, desmopressin reuse will help to establish the diagnosis of non-transient DI. A genetic test may help to differentiate the aetiology of DI in our index case and establish whether it was secondary to HIE versus familial.
Conclusion
The quick weaning of desmopressin since the commencement of sodium valproate in our case, suggests that sodium valproate may have contributed to the improvement in DI symptoms. We propose that sodium valproate can help in the treatment of DI by increasing the production of ADH. Clinicians using sodium valproate for the management of seizures in neonates with concurrent DI need to bear in mind this potential side effect of sodium valproate.
The differential diagnosis of familiar neurohypophyseal DI cannot be ignored in our index case because of the strong family history of DI. The review of investigations (eg serum osmolality paired with urine osmolality, urine output, serum sodium, blood glucose, cortisol, thyroid stimulating hormone, adrenocorticotrophic hormone) along with detailed reporting of brain MRIs (including commenting on the pituitary gland) usually help in establishing a diagnosis of DI.
Parental consent
The authors are grateful to the parents for consenting to the writing of this case report.
Or read this article in our
Tablet/iPad edition
- This case of DI presented a dilemma: was it DI secondary to hypoxic ischaemic encephalopathy or familial DI?
- Neonatologists should consider the possible effect of sodium valproate in increasing ADH secretions when used to treat seizures in a neonate with DI.
Also published in Infant:
