

An unusual case of refractory hypotension in an extremely preterm baby
Intra-abdominal birth trauma is an uncommon yet severe and life-threatening event. Direct or indirect trauma of an abdominal organ during birth could lead to abdominal haemorrhage in the newborn infant. We present the case of a preterm infant with a subcapsular haematoma of the liver. This lesion should be suspected in infants with unexplained anaemia, hypovolaemia or haemodynamic instability.
Vipul Bhaskar1MBBS, MD (Paediatrics), MTI Fellow (Neonatology)
Srinivasarao Babarao2
MBBS, MD (Paediatrics), DCH, MSc, FRCPCH;
Consultant Neonatologist
Sanjeev Rath1
MBBS, MD Paediatrics (PGIMER), FRCPCH;
Consultant Neonatologist
Pek Wan Lee1
MBBS, MRCPCH, FRCPCH;
Consultant Neonatologist
1Arrowe Park Hospital, Wirral
2Liverpool Women's Hospital
The case report
An extreme preterm baby boy was born at 25+5 weeks’ gestation through spontaneous vaginal delivery weighing 715g. Antenatal steroids and magnesium sulphate could not be given as the mother rapidly delivered the baby within 30 minutes of presentation. The baby was born in poor condition requiring intubation, surfactant administration and ventilation. As the hypoxia got worse, nitric oxide was commenced.
Blood investigations on admission indicated profound anaemia (haemoglobin = 107g/L), for which the baby received 10mL/kg of emergency O-negative blood soon after birth at about one hour of age. The cause of the anaemia was initially thought to be the extensive bruising observed on the face and scalp.
The infant remained haemodynamically unstable with low mean arterial blood pressure. He received one normal saline bolus at 10mL/kg at about three hours of age. He needed support with multiple inotropes (dopamine, dobutamine, hydrocortisone and adrenaline) yet his clinical condition remained unstable and critical. Despite maximum inotropic support, the arterial blood pressure remained low at 15mmHg during the first 4-6 hours of life. There was very little response to the fluids and escalation of inotropic support.
He received two packed red blood cell transfusions at 15mL/kg each in the first 12 hours of life. He had refractory metabolic acidosis with base deficit in the range of -16 to -24mEq/L and high lactate concentrations in the range of 13 to 22mmol/L. The infant received multiple sodium bicarbonate corrections within the first 12 hours of life in an attempt to correct the acidosis. His coagulation profile was deranged (prolonged activated partial thromboplastin time, APTT=110secs; high international normalised ratio, INR=3.0; low fibrinogen=0.6g/L; high D-dimer >5000ng/mL) and he was treated with vitamin K, fresh frozen plasma and cryoprecipitate within the first 12 hours of life.
Antibiotics were appropriately started to empirically manage a sick preterm baby. C-reactive protein (CRP) levels were unremarkable. Blood cultures remained negative. Clinical examination revealed a flat and non-discoloured abdomen.
Cranial ultrasound was performed at 8 hours of life to look for intraventricular haemorrhage (IVH). This showed a grade 2 IVH on the left side only, which was unable to explain the critically unstable clinical state of the preterm neonate with severe anaemia, refractory hypotension and metabolic acidosis.
The poor response to multiple fluid boluses, blood products and inotropes made the team consider the possibility of suboptimal central line position/extravasation but radiological imaging showed the central lines in optimal positions.
Despite full aggressive medical intervention, his anaemia, hypotension and metabolic acidosis remained refractory and the neonate continued to be in a very unstable and critical condition. A third packed red blood cell transfusion was ordered but following discussion with the family, his care was redirected to palliation at approximately 18 hours of life due to persistent hypotension, worsening metabolic acidosis and poor response to active intensive care management. The baby died at 19 hours of age.
A post mortem was conducted as the cause of death and non-refractoriness of the hypotension and metabolic acidosis to multiple treatments was not clear. The post mortem examination revealed a ruptured subcapsular haematoma of the liver with haemoperitoneum (FIGURE 1).
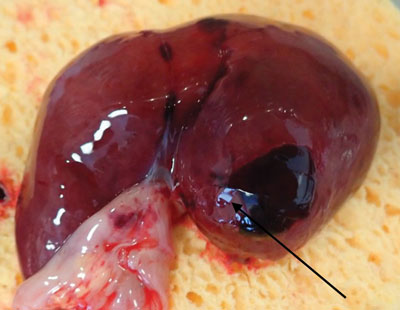
FIGURE 1 Sub-capsular haematoma of the liver. The arrow shows the site of the rupture.
The case was subjected to an internal mortality review and Perinatal Mortality Review Tool (PMRT) review. The grading of care for this baby was considered to be grade A (no issues with care identified from birth up to the point at which the baby died).
Review and discussion
The overall incidence of birth injuries is approximately 2% and 1.1% in singleton vaginal and caesarean deliveries, respectively.1,2 Risk factors that can increase the risk of birth injuries include:
The baby discussed in this case report was born prematurely at 25+5 weeks’ gestation by spontaneous vaginal delivery; prematurity was the only risk factor.
Intra-abdominal birth trauma is uncommon and primarily consists of rupture or haemorrhage in the liver, spleen or adrenal glands.3,4 The clinical presentation of intra-abdominal trauma is dependent upon the amount of blood loss:
- infants with hepatic and splenic rupture may present with sudden onset pallor, signs of haemorrhagic shock, abdominal distension and discoloration
- infants with subcapsular haematoma may have a delayed or more insidious onset of symptoms of anaemia and shock, which includes poor feeding, tachycardia and tachypnea
- unilateral adrenal haemorrhage may present as an abdominal mass.
In our index case there were no risk factors suggestive of intra-abdominal birth trauma except for prematurity. The abdomen was not discoloured or distended; it looked flat, if not sunken (scaphoid), and hence it was challenging for the team to consider abdominal birth trauma as a possibility for the clinical presentation. The infant did not have tachypnea or tachycardia; he had poor respiratory efforts and remained ventilated throughout his stay.
The cause of anaemia in our case was initially presumed to be the extensive bruising of the face and scalp, which comprises a significant part of body surface area in an extreme preterm baby. The grade 2 IVH on the left side only did not correlate with the baby’s condition. Suboptimal central line position/extravasation may have been the reason for the poor response of the metabolic acidosis and hypotension to the respective interventions, however, this possibility was ruled out.
The post mortem in our index case showed a ruptured subcapsular haematoma in the liver with haemoperitoneum. The condition appeared as hepatic and splenic rupture with signs of haemorrhagic shock but unusually, there was no abdominal distension and/or discoloration.
The incidence of subcapsular haematoma of the liver is very low in infants and diagnosis may be delayed or missed. Some cases of subcapsular haematoma of the liver have been incidentally found on ultrasonography.5 The diagnosis is frequently made at autopsy.6
Proposed predisposing factors for subcapsular haematoma of the liver include prematurity, very low birth weight, sepsis, hypoxia, pneumothorax, traumatic labour, traumatic umbilical venous catheterisation, cerebral haemorrhage, coagulopathies, and exposure to drugs that lead to bleeding.7 The three main causes of subcapsular haematoma of the liver are fragility of the neonatal liver, trauma and coagulopathy. Most reported cases are in babies born premature or at very low birth weight. It is believed that in these infants the liver has a weaker connective tissue framework and poor contractility of hepatic veins, which increases the risk of trauma.8 Stretching of attached hepatic ligaments during delivery may induce liver laceration.5
Conclusion
From the case presented, we conclude that a ruptured subcapsular haematoma of the liver/spleen can present in a preterm baby as refractory anaemia, hypotension and metabolic acidosis without abdominal findings on clinical examination. It should be considered in the differential diagnosis when response to management is poor and other common causes (for example, large IVH, central line extravasation, etc) are ruled out. Bedside abdominal ultrasound scanning in such cases could help to delineate the lesion and establish a rapid diagnosis.
Parental consent
The authors received consent to publish this report from the patient’s parents.
Or read this article in our
Tablet/iPad edition
- Even without evidence of birth trauma, intra-abdominal bleeding must be suspected in a newborn infant with refractory hypotension.
- Early identification of the source of bleeding may improve the outcome.
- Ultrasonography is the best modality to diagnose intra-abdominal birth injuries and can be performed at the bedside.
Also published in Infant:
