

Developments in allied health professionals’ role in UK neonatal units: a speech and language therapy perspective
The recent Getting It Right First Time (GIRFT) survey (2019) has highlighted the significant lack of allied health professional (AHP) provision in neonatal care in the UK. Speech and language therapists (SLT) are part of the AHP workforce currently under-represented in neonatal care. This article summarises how SLTs are addressing the feeding and early communication service requirements and SLT skills needed to support newborn infants and families, and contributing to the wider multidisciplinary neonatal care team.
Rebecca MurphyHighly Specialist Speech and Language Therapist, Evelina London Children’s Hospital
rebecca.murphy2@gstt.nhs.uk
Celia Harding
Honorary Professor, City University London and Honorary Speech and Language
Therapist, Royal Free NHS FT
Annie Aloysius
Clinical Specialist Speech and Language Therapist (Neonatology), Imperial College Healthcare NHS Trust
Michelle Sweeting
Neonatal Speech and Language Therapist, Mid & South Essex Hospitals NHS FT
Siew-Lian Crossley
Highly Specialist Speech and Language Therapist, formerly Homerton University Hospital NHS FT
Background
Approximately 90,000 infants born in the UK each year are provided with some form of specialist support from neonatal care.1 Depending on the gestational age at birth and specific medical needs of an infant, care is provided in one of three levels of unit: level 3 neonatal intensive care unit (NICU), level 2 local neonatal unit (LNU) and level 1 special care unit (SCU). Each level offering specific services to meet the needs of infants with varying developmental and medical requirements.2 Preterm and term infants, who need additional support post birth, often require medical care and support from allied health professionals (AHPs) both within a neonatal unit and when discharged home.3
In recent years, neonatal care has included AHPs who have evolved discipline-specific roles as part of the neonatal team. Development of guidance3 identified the importance of the speech and language therapist (SLT) in supporting early feeding and communication skills, and this has led to increased funding and positions for SLTs in neonatal care. The SLT role has continued to develop with an increased focus on maximising positive benefits for preterm infants and their families, with an emphasis on early interaction and the feeding relationship in improving these outcomes.
The recent summary document of neonatal services and workforce in the UK from the GIRFT and Royal College of Paediatrics and Child Health (RCPCH) assessment data4 highlighted the significant shortage of medical and nursing staff in neonatal services across the UK. AHPs were found to be available in less than half of UK neonatal units during the week and almost completely absent at weekends. As a result, NHS trusts have been asked to develop an AHP strategy as part of workforce planning, to identify the level currently available and expertise needed, and how any gaps identified can be filled. Operational Delivery Networks (ODNs) with support from NHS providers, maternity clinic networks and local maternity services will identify where action needs to be taken at ODN level and there are plans and funding available to establish ODN AHP posts.5
SLTs are part of the AHP workforce currently under-represented within neonatal care. SLTs work in collaboration with members of the neonatal team in the areas of feeding, swallowing and early communication.6 This article summarises the contribution of the Royal College of Speech and Language Therapists (RCSLT) SLT Neonatal Clinical Excellence Network (CEN) in recent years and considers future challenges and recommendations.
The function of the RCSLT SLT Neonatal CEN
The RCSLT supports CENs across a range of lifespan clinical disorders to provide peer support within clinical specialties, and to enable meetings and conferences to discuss the best available evidence to support therapeutic interventions and encourage research and best practice. In July 2014, a national meeting for SLTs working in neonatal units across the UK was held with the support of the RCSLT. The meeting was an opportunity for SLTs working in neonatal units to share practices, pool and map resources and come together with RCSLT to see how to move the profession forward in neonatal care. The meeting was a success and led to the development of a neonatal working party with associated working groups.
The RCSLT SLT Neonatal CEN was formally established in 2018 to provide a forum for SLTs in the UK working within neonatal care and those who follow up preterm infants in the community. SLTs currently are often lone workers or work within a small SLT team supporting neonatal care and the CEN can therefore provide an important source of support. In addition, CENs support participation with and provision of advice to associated professional organisations (eg the British Association of Perinatal Medicine, BAPM), contributing to relevant multidisciplinary policies and workforce planning, which impact on the provision of SLT. CEN members also participate in consultations and project work in the areas relevant to early feeding and communication with charitable organisations such as Bliss and Best Beginnings. When necessary, the CEN provides position statements to address complex issues that have implications on clinical practice and outcomes. TABLE 1 highlights the key standards and policies that members of the SLT Neonatal CEN have participated in and contributed towards.
TABLE 1 Key standards and policy documents that CEN members have participated in.
The CEN recognises that being aware of the best evidence to support and promote infant feeding and communication is necessary to enable SLTs to provide the best methods of assessment and intervention. All therapeutic work is undertaken with the understanding that working with a team within a developmental care framework is essential. An annual Hot Topics conference is hosted by City, University of London, where the most relevant evidence of the previous year is presented, and invited speakers disseminate and discuss new innovations and practice. There is a direct focus on research undertaken by SLTs both in the UK and from around the world. This forum also promotes discussion of research ideas, National Institute for Health Research (NIHR) grant proposals, current research projects and service evaluations. Many CEN members have undertaken research that is highly relevant to improving clinical interventions and published in peer reviewed journals. Publications have investigated pertinent clinical topics including:
- use of non-nutritive sucking7-9
- screening to identify neonatal feeding problems10
- clinical considerations when feeding infants on high flow nasal cannula oxygen11
- investigating bottle teat flow rates on neonatal units12
- infant communication on neonatal units13
- the impact of prolonged use of masks when caring for infants during the COVID pandemic.14,15
The CEN has four key working groups committed to developing and supporting neonatal SLT.
1. National neonatal SLT provision; benchmarking and implementing national staffing and practice standards
Between October 2016 and October 2017, the CEN, with support from the RCSLT, undertook a national benchmarking survey of SLT provision across UK neonatal units. The questionnaire surveyed the level of care, funding, banding, clinical experience, clinical supervision, training, multidisciplinary team composition and the nature of therapeutic interventions provided. Data were returned from 67 (35%) units. Many units did not have a SLT service and there was a higher response rate from units that did. Most responses (93%) were from level 2 (LNU) and 3 (NICU) units. SLTs working on neonatal units demonstrated a wide range of clinical experience, from less than a year to more than 10 years, with 71% of the sample indicating more than six years working in neonatal care. Funding for SLT posts on units was sourced from a variety of financial options as shown in FIGURE 1.
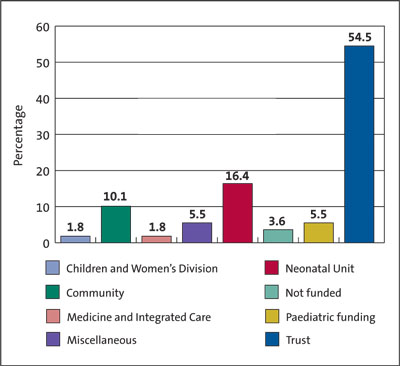
FIGURE 1 Funding sources for SLT posts in neonatal care. The term ‘not funded’ refers to services that access a SLT from another provision to provide assessment and intervention on an ad hoc basis.
From the survey, it was identified that 54% of units had allocated time for SLTs to work on the neonatal unit. Differences in funded provision varied between levels of unit, with level 3 (NICU) units having more funded provision and level 1 (SCU) the least. Banding of SLT posts within each level varied from 6 to 8c. Most SLTs (85%) had clinical support and supervision, 71% had support from therapists skilled in neonatal care. Band 6 SLTs worked with support from a higher banded SLT.
Reasons for referral to SLT are indicated in FIGURE 2. Requests to assess safety of the swallow was the most frequent reason for SLT input.
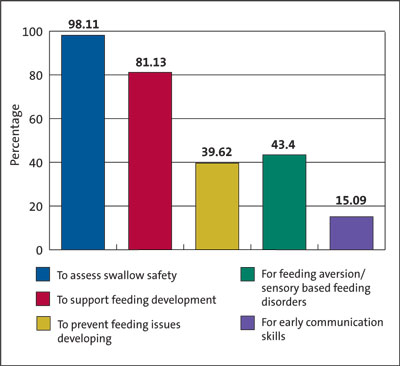
FIGURE 2 Reason for referral to SLT.
These findings highlighted significant variation in delivery, support and supervision for SLT provision to neonatal services. Aside from practical aspects of intervention and support for infants and their families, problems with establishing team working, specifically with other AHPs because of limited allocation of time was cited as a problem in enabling growth and development of a post and providing an embedded proactive rather than reactive service. From these data, the CEN developed the RCSLT SLT Staffing Recommendations for Neonatal Units document (2018)16 later used as part of the GIRFT NHS improvement initiative.
The GIRFT programme aimed to support the implementation of the Neonatal Critical Care Transformation Review (NCCTR), which recommended neonatal networks and services produce a gap analysis looking at staffing. The GIRFT survey, carried out in 2019, highlighted the significant lack of AHP provision on neonatal units nationally. In response to GIRFT results and NCCTR recommendations, members of the CEN updated the original benchmarking data (2017) and produced a gap analysis comparing current SLT provision to the RCSLT SLT neonatal staffing recommendations.16
This gap analysis helped highlight specific deficits in SLT provision to enable the further establishment of required SLT posts in relation to the number of cots and level of unit. Taking this work forward will be a key focus for newly established neonatal ODN SLTs.
2. Education and training
Access to training and development opportunities for SLTs working in neonatal care has been inconsistent with training opportunities ranging from therapists accessing formal neonatal courses to in-house training and development. There is a need for access to more specific training opportunities for SLTs in order to build skills in this area and strengthen the profession moving forward. The bench-marking survey revealed a lack of structure and standards to enable neonatal SLT workforce planning. It highlighted both the need to develop a competency framework for neonatal SLT and the educational opportunities to achieve delivery.
The RCSLT dysphagia framework is comprehensive, but there was a need for specific competencies for this specialist area of dysphagia in order to ensure that all SLTs working in neonatal care have the competence and confidence to support these complex infants and their families. Neonatal competencies were developed with the support of RCSLT to make the skills and knowledge required for SLTs clearer and support managers in service development and recruitment. Competencies also ensure a skilled work-force in this area and strengthen the role of SLTs in neonatal units.
All undergraduate SLTs leave university with a basic knowledge of dysphagia across the lifespan. Neonatal SLT education and skills are undertaken at post-basic, postgraduate level. Currently educational requirements are enabled through access to ad hoc study days from specialist SLTs or conferences and courses provided by organisations, such as National Association of Neonatal Therapists, Bliss, Brazelton Centre, and the Newborn Individualized Developmental Care and Assessment Program (NIDCAP). In addition, many qualified clinicians provide postgraduate support, with use of competencies to structure and guide skill acquisition.
The annual Neonatal CEN Hot Topics study days were established in 2018 to further meet the need for continued professional development in this specialist area.
Education is a current area of focus for the CEN. We are embarking on a joint project with Health Education England and e-Learning for Healthcare to develop the foundation and clinical expert/specialist level clinical competencies curriculum and resources.
3. Outcome measures
Outcome measures are an important part of the SLT role, to demonstrate effective patient care and improve quality of care. The working party has identified that while it is important for SLTs to be able to show the effectiveness of what they do, it is challenging to find one tool or model that encompasses the breadth of the neonatal SLT role. The role of the SLT in neonatal care is varied: from direct work with infants with feeding and swallowing impairments, to working with families and the medical, nursing and AHP team to support and improve feeding and communication outcomes. In order to measure outcomes of SLT interventions in neonatal care there may be the need for a suite of tools or a multifaceted tool that looks at SLT, parent and neonatal staff measures.
The outcome measures group is investigating and evaluating current outcome measure tools. The TOMS (therapy outcome measures) paediatric dysphagia scale is of use with infants with feeding impairment.17 Two TOMS scales are in development: one which assesses parent-infant responsiveness and another that focuses on infant pre-feeding skills. These have been trialled but did not capture the breadth and specific input of neonatal SLT provision. A tool is currently in development and being trialled by CEN that considers seven domains of neonatal SLT input and outcomes.
4. Communications
To enable SLT neonatal colleagues to share and receive information from CEN working groups, projects, pending courses, clinical queries, job opportunities and research relevant to neonatal care, the RCSLT has provided a Basecamp (an online project management tool) protected site. In addition to this, the RCSLT website has been updated to make it easier to find CEN moderated information pertinent to neonatal SLT care. Currently these resources are available to RCSLT members only. We are working with BAPM to provide wider access to information on neonatal SLT via its open access website.
The CEN’s presence on social media platforms, Twitter and Facebook, provide other methods of sharing research published from around the world as well as a means of supporting contact between SLTs and other neonatal professionals.
Conclusions
The neonatal workforce is currently in a critical phase of development, with AHPs particularly under-established and under-represented.4 Core skills required of a SLT are defined within the 2010 BAPM Service Standards,6 and these skills are appropriate for all levels of neonatal unit. However, to ensure that SLT skills are fit for purpose and continue to progress and meet the needs of infants and families receiving neonatal care, the CEN is committed to the following actions:
- ongoing contributions with RCSLT and university establishments that train SLT students to ensure that training for dysphagia meets the needs of probationer SLTs on graduation, and that postgraduate training reflects the clinical competencies and advanced skills required for neonatal care
- to work closely with Health Education England to develop equitable and accessible training and career progression for SLTs specialising in neonatal care to ensure the workforce has the expert skills required and there is succession planning while growing the workforce
- development of the neonatal SLT operational delivery network role
- ongoing review of SLT service provision, with audit of the Speech and Language Therapy staffing Recommendations for Neonatal Units document16
- investigation of the diversity of therapeutic skills required for each level of unit aside from the core skills identified6
- ongoing support for research projects from CEN members, with increased efforts to link to universities for additional support
- ongoing contributions and participation in any future policies and procedures which impact on neonatal care
- ongoing support and peer support for CEN members, with opportunities to share successful work projects and activities
- to establish a robust outcome measure tool that captures the breadth of the neonatal SLT role
- developing and enhancing collaboration with other AHP groups and professional bodies specialising in neonatal care across the UK to support service development, continued professional development and inform national standards and policies.
Acknowledgements
The authors’ thanks are extended to members of the Speech and Language Therapy Neonatal CEN committee, in particular Jo Marks, Professional Lead for Speech and Language Therapy, Royal Manchester Children’s Hospital.
Or read this article in our
Tablet/iPad edition
- SLTs are core members of the neonatal team.
- SLTs work collaboratively within the neonatal team to support early infant feeding and communication skills.
- SLTs are contributing to current workforce developments in neonatal care.
Also published in Infant:
