

Therapeutic hypothermia for neonatal encephalopathy: what’s new in BAPM’s latest framework for practice?
Since the British Association of Perinatal Medicine (BAPM) published its Position Statement on Therapeutic Hypothermia (TH) for Neonatal Encephalopathy in 2010, TH has become firmly established as the standard of care for all term infants with moderate or severe hypoxic-ischaemic encephalopathy (HIE). There is increasing evidence of its long-term benefits for these infants, as well as its cost-effectiveness.1 The new BAPM Framework published in November 2020 therefore expands upon the previous guidance and incorporates the most up-to-date evidence.
Kathryn MacallisterNeonatal Grid Trainee, St Michael’s Hospital, Bristol
k.macallister@nhs.net
Steve Jones
Consultant Neonatologist, Royal United Hospital Bath, and BAPM Executive Committee representative for South of England
Ela Chakkarapani
Consultant Neonatologist and Senior Lecturer in Neonatology, University of Bristol
On behalf of the BAPM Therapeutic Hypothermia for Neonatal Encephalopathy Group
Neonatal hypoxic-ischaemic brain injury has potential life-long implications for babies and their families, so timely initiation of interventions that can improve outcomes is essential. It is hoped that this framework will be used as a basis for local and network guidelines in the UK, allowing for more streamlined care pathways and assisting with consistent decision-making and referrals between special care units (SCUs), local neonatal units (LNUs) and neonatal intensive care units (NICUs).
This article focuses on how the framework addresses cases where infants do not meet all of the criteria for TH, which results in uncertainty as to whether to offer this treatment or not. In addition, it discusses the vital role of neonatal networks in the TH pathway, as not only is a transport team required to transfer cooled infants to a NICU in a timely fashion, but networks also have a responsibility to ensure adequate training and provision of equipment in all units in the network. Regular clinical governance reviews of cases and practices will be essential to ensure the highest quality of care is offered in all neonatal networks.

Baby undergoing aEEG monitoring.
Which infants should be cooled?
Any infant of at least 36 weeks’ gestation with evidence of moderate or severe encephalopathy on clinical examination within six hours of birth following significant perinatal hypoxia-ischaemia should be considered for TH. Ideally an amplitude integrated electroencephalogram (aEEG), also referred to as cerebral function monitoring (CFM), should be used to confirm the clinical diagnosis of encephalopathy and guide this decision making. However, lack of availability of aEEG should not prevent or delay treatment.
The eligibility criteria for TH are based on the original TOBY study2 and assessed as criteria A, B and C (FIGURE 1). Infants must fulfil at least one ‘A’ criterion to demonstrate significant perinatal hypoxia-ischaemia and must also have evidence of significant neonatal encephalopathy, as described in the ‘B’ criteria. These infants should commence aEEG monitoring and should undergo TH if there is evidence of seizures or abnormal background aEEG activity (criteria ‘C’).
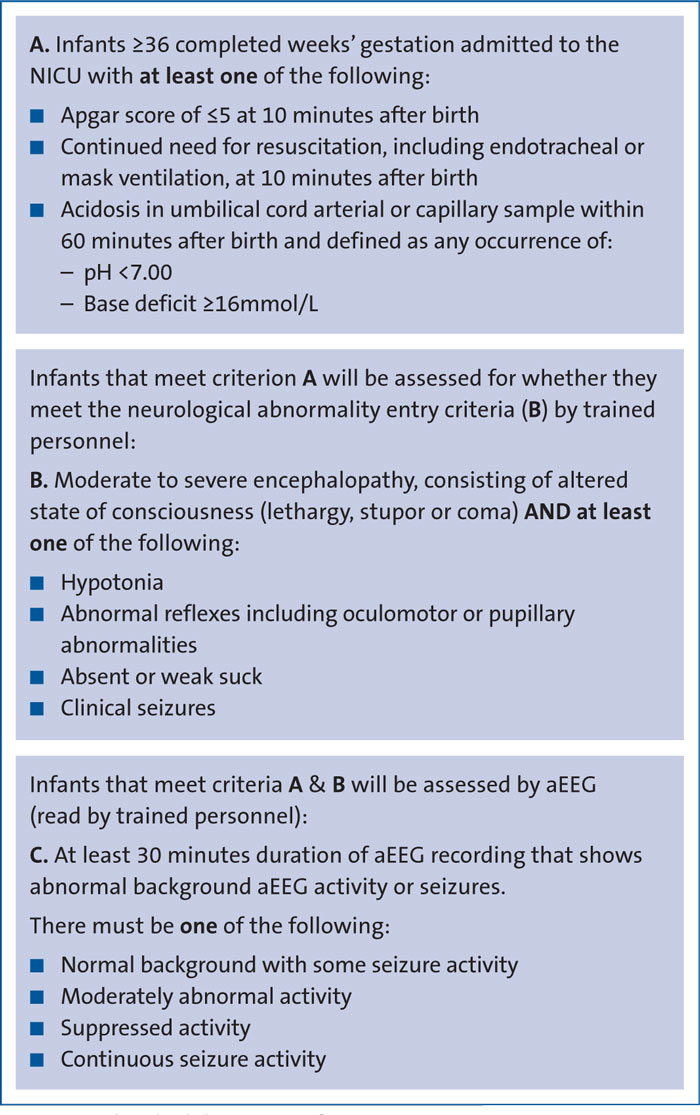
FIGURE 1 The eligibility criteria for TH.
While the criteria recommend at least 30 minutes of abnormal aEEG prior to initiating TH, it may be clear in infants with suppressed aEEG activity or continuous seizure activity that the criteria have been met after 10 minutes of monitoring and TH should not be delayed. aEEG provides additional information that is less subjective than clinical examination, can be independently assessed remotely by staff with neurological expertise and provides more continuous assessment for changes in condition of the baby. If aEEG monitoring is not available then it is appropriate to begin cooling those infants who are clearly encephalopathic with abnormal neurological signs, providing they have been assessed by a suitably trained practitioner. It is important that we do not cool babies who do not need TH as this results in unnecessary separation of mother and baby with associated adverse impacts on parental mental health, significant intensive care interventions for the baby and exposure to the risk of potential complications from TH.
Benefits of TH
Without TH, the risk of death or severe disability following moderate HIE is approximately 25%, and in severe HIE this rises to around 75%.3-5 A systematic review has shown that TH to a core temperature of 33-34°C initiated within six hours of birth and continued for 72 hours reduces death and disability at 18 months of age in infants with moderate or severe HIE.6
TH improves neurocognitive outcomes at school age, reducing the rates of cerebral palsy and moderate or severe disability as well as improving the proportion of survivors with intelligence quotient (IQ) scores >85.3 Rates of epilepsy are also reduced following TH.7
Initiation of TH
Cardiorespiratory stability takes precedence over TH, so cooling should only be commenced once any initial resuscitation has been undertaken and adequate heart rate and oxygen saturations have been achieved.
TH without intracorporeal temperature monitoring is not recommended by NICE (The National Institute for Health and Care Excellence) and all infants commencing any form of TH, including switching off the heater on the resuscitaire, should have their temperature continuously monitored, ideally using an intracorporeal temperature probe, such as a rectal probe. Infants being assessed for TH while maintaining normothermia or passive hypothermia must have continuous temperature monitoring to prevent hyperthermia or hypothermia below 33.5°C. Hyperthermia is associated with increased brain injury in animal models of hypoxia-ischaemia and in infants with HIE8,9 and must be avoided in all infants with suspected HIE.
Ongoing TH should be achieved using a servo-controlled cooling device to maintain a core temperature of 33.5°C. TH is an intensive care activity and as such all infants undergoing TH must be cared for in a NICU. The appropriate referrals should be made as soon as the need for TH is confirmed. In cases where there is uncertainty around eligibility for TH, it is recommended that infants are discussed with the local cooling centre for further guidance. These discussions must be had promptly to ensure that TH is commenced as soon as possible where it is deemed appropriate, ideally within three hours of birth.
Cooling infants outside of the criteria
Infants <36 weeks’ gestation
While no current randomised controlled trial data exist to support the use of TH in infants <36 weeks’ gestation, many centres have offered TH to selected infants from 33-35 weeks. Data published in a case series suggest that long-term outcomes for these infants following cooling may be comparable to those for infants over 36 weeks,10 but that there may be a higher risk of complications and of the need to rewarm before completion of 72 hours of TH in the more preterm infants.11 Where TH is considered in these infants, it is recommended that a second opinion is sought from an experienced consultant and a detailed discussion of the risks and potential benefits is held with the parents and documented. The Preemie Hypothermia for Neonatal Encephalopathy trial in the US has randomised 33-35+6 week infants to TH or standard care and initial results should be available in late 2022.
Mild encephalopathy
A 2020 systematic review found that at present there is insufficient evidence to recommend cooling for this group of infants and that harm from TH cannot be excluded.12 A thorough neurological assessment by an experienced practitioner is essential to identify those infants with no more than mild encephalopathy, and at present cooling would not be recommended for these infants outside of clinical trials. It is worth noting that more infants with moderate encephalopathy are being cooled worldwide than were entered into the original TH trials and there appears to be a shift towards cooling infants with milder encephalopathy, which is not supported by current evidence and has important resource implications.
Infants over six hours of age
Infants where perinatal hypoxia-ischaemia is suspected but who have a normal neurological examination at birth should be carefully assessed during the six hours after birth to allow initiation of TH if their condition changes. Despite this, infants sometimes present after six hours of age with presumed HIE and clinicians may decide to cool these infants in the absence of any evidence of harm from cooling at this time point. However, the evidence of benefit of TH initiated 6-24 hours after birth is modest,13 emphasising the importance of commencing cooling within six hours wherever possible, and ideally within three hours of birth.
Sudden unexpected postnatal collapse
There is currently no randomised controlled trial evidence to support the use of TH in infants with signs of moderate or severe encephalopathy following a postnatal collapse. The aetiology of postnatal collapse is very varied and it is vital that the underlying cause is considered before initiating TH in case there may be adverse risks associated with cooling. However, one cohort study showed that long-term outcomes for cooled infants who did not meet the standard inclusion criteria, including those cooled following postnatal collapse, were similar to the outcomes for those who met the standard inclusion criteria, suggesting that TH may have some potential benefit for those infants who collapse postnatally.10 In addition, many of the animal models of neonatal hypoxic-ischaemic insults that have been used to demonstrate the effectiveness of TH involve a postnatal insult, indicating that the protective effects of TH may extend to postnatal insults. If TH is considered appropriate, it is recommended that this is discussed with a second experienced consultant and a detailed discussion of the risks and potential benefits is held with the parents and documented before a decision is reached.
Family-integrated care and communication with parents
Parents should be encouraged to be present with their infants while undergoing TH and family-integrated care should be facilitated where possible. Where the infant has to be transferred between hospitals, the mother should be transferred as soon as possible and separation should be minimised. Mothers should be encouraged to express breast milk that can be used for mouth care, and trophic feeds should be considered if there is no ongoing organ dysfunction.
Open communication with parents is essential from the moment a diagnosis of HIE is suspected and parents should receive timely updates which are sensitive and honest. They may need information to be repeated more than once or delivered in a different format.
Parents may have questions about their antenatal and intra-partum care, as well as their infant’s neonatal care, and they should be offered follow-up with appropriate professionals to discuss this. There should be a multidisciplinary review of the perinatal and neonatal care in cases where the infant underwent TH, and parents should be informed of this and have the opportunity to contribute and to be updated with any outcomes.
Prognosis
The possible outcomes for their baby are of vital importance for parents and there are a number of factors that can be used to inform prognosis, including the evolution of neurological exam-ination, aEEG activity and magnetic resonance imaging (MRI) findings. The prognosis should be classified as high, moderate or low risk of significant neurodevelopmental impairment based on these factors.14
Regular neurological examination is essential, but this is influenced by TH itself as well as by medications such as sedatives and anti-convulsants.15 TH affects the metabolism of many drugs and it may take longer than expected for any suppressive effects to subside. Clinicians must take this into account when using clinical examination or aEEG activity to assess prognosis, ensuring that any medications administered have had adequate time to be metabolised and excreted.
aEEG monitoring should be continued throughout TH until the end of rewarming and may help with recognition of seizures and assessment of prognosis. The aEEG activity should be regularly documented and the timing of any return to normal activity should be recorded.
All infants undergoing TH should have an MRI scan between five and 15 days after birth, preferably between days 5 and 7. Rutherford et al analysed MRI findings and outcomes at 18 months for infants enrolled in the TOBY trial and found that lesions in the basal ganglia, thalami, posterior limb of the internal capsule and white matter were able to accurately predict outcomes at 18 months of age for both cooled and non-cooled infants.16
Where possible, proton (1H) magnetic resonance spectroscopy (MRS) lactate/N-acetyl aspartate (Lac/NAA) of the basal ganglia and thalamus should be performed alongside the MRI as this is the most accurate predictor of outcome in babies who have undergone TH. Azzopardi et al studied 62 infants who underwent TH and who were available for follow-up at 2-3 years of age, showing that the Lac/NAA ratio in the thalamus and fractional anisotropy in the posterior limb of the internal capsule measured within 15 days of birth were accurate predictors of the presence of moderate or severe disability at 2-3 years of age.17
Prediction of outcomes based on MRI and MRS can be helpful to provide parents and other services with information to help plan ongoing care. However, clinicians must be aware that the actual outcomes can vary significantly between individual infants and must be able to communicate this uncertainty to parents.
If clinical signs suggest a very poor prognosis before day 5 then an MRI may be obtained early to support clinical judgement and guide discussions with parents. Studies have shown that an MRI on day 2-3 of TH can accurately define the presence and extent of injury seen on a day 10 MRI, whereas an MRI performed on day 1 may be too early to define the full extent of injury.18
Prognosis should be discussed with parents before discharge from the NICU and summarised in written communication to parents and other healthcare professionals including those in the referring unit and in primary care.
Governance
In all cases where TH is considered, there should be clear, contemporaneous documentation of decision making, whether TH is initiated or not. This should include documentation of neurological examination, aEEG and discussion with parents. Given the proven benefit of TH and its safety, formal consent from parents is not required but it is important that parents are fully informed and that their views are taken into account. There should be peer review of all cases that are assessed for possible TH.
As discussed previously, there should be a multidisciplinary review of perinatal and neonatal care in all cases where an infant undergoes TH, focussing particularly on avoidable factors, the appropriateness of TH and the timeliness of its initiation.There should be a mechanism to disseminate learning from these reviews.
There should be formal logs of training and competence in the skills of standardised neurological examination and aEEG interpretation, organised at a network level where possible.
There should be regular network-wide audit of all cases of TH and neonatal encephalopathy and regular benchmarking, using consistent criteria and definitions of HIE to allow identification of trends and any outliers.
Implications for neonatal networks
The decision to commence TH must be made promptly by a practitioner who is competent to assess whether a baby meets the criteria for TH. All SCUs, LNUs and NICUs should be able to assess infants using aEEG and initiate TH using servo-controlled cooling equipment. Neonatal networks should facilitate the provision of equipment and training to improve the recognition of neonatal encephalopathy and initiation of TH, including training in neurological assessment and aEEG interpretation. Referral pathways for TH within the network must be clear and, where there is uncertainty around the diagnosis, early discussion with a senior clinician at the local cooling centre is recommended.
Once TH has been initiated, infants should be transferred to an appropriate NICU by an established transport service that is able to provide servo-controlled cooling therapy during transport. Where aEEG is not available in the referring unit, the transport team should consider taking portable CFM with them to assist diagnosis. Networks should explore remote review of aEEG and the use of telemedicine to support decision making in referring units.
At sites where there are no on-site paediatric services, such as stand-alone midwifery led units, staff should be trained to recognise infants who may benefit from TH but should not initiate TH in such settings. Infants should be transferred along the normal referral pathway for sick infants, appreciating the need for prompt referral and transfer as an emergency so that TH can be started as soon as possible where it is indicated. Maintenance of normothermia and avoidance of hyperthermia is vital, and regular clinical observations are required, along with blood glucose monitoring.
Conclusion: key learning points
- TH remains the only evidence-based intervention for moderate or severe neonatal encephalopathy. All maternity units with paediatric cover should have equipment and skills to identify and initiate treatment including aEEG and servo-controlled cooling equipment.
- Neonatal networks must not only provide clear pathways for the transfer of any infants undergoing TH to an appropriate NICU, but should also ensure provision of adequate training to staff and monitoring of their competencies in neurological examination, aEEG application and interpretation, as well as provision of equipment for all SCUs, LNUs and NICUs to allow TH to be commenced as soon as possible in appropriate cases.
- There are a number of instances where it may be appropriate to cool infants who do not meet all of the criteria for cooling, but in the face of limited evidence this decision must always be made by the most experienced clinicians and should involve a clear discussion of the risks and benefits with the parents.
- Communication with parents must be timely, open and honest, reflecting the significant degree of prognostic uncertainty that often exists.
Acknowledgements
The BAPM Therapeutic Hypothermia for Neonatal Encephalopathy Group: Eleri Adams, Consultant Neonatologist; Topun Austin, Consultant Neonatologist; Julie-Clare Becher, Consultant Neonatologist; Kate Dinwiddy, Chief Executive, BAPM; David Edwards, Consultant Neonatologist; Shona Elliot, Parent Rep, Peeps HIE charity; Kelly Harvey, ANNP; Jane Hawdon, Consultant Neonatologist; Sarah Land, Charity Manager, Peeps HIE; Janet Rennie, Consultant Neonatologist; Nikki Robertson, Consultant Neonatologist.
Or read this article in our
Tablet/iPad edition
