

Shared decision making: translating guidance into practice
In 2019, the British Association of Perinatal Medicine (BAPM) updated its existing document on consent as a framework on enhancing shared decision making in neonatal care. This framework reflects the increasing emphasis on the role of parents in neonatal care, the decline of medical paternalism in health care and the increasing emphasis of parental involvement in neonatal clinical decision making. This article provides a summary of the main areas in the BAPM framework, how it aligns with the new GMC guidance and some practical tips for how neonatal healthcare practitioners can translate guidance into clinical practice.
Jennifer McGrathConsultant Neonatologist, St Peter’s Hospital, Chertsey, Surrey
jennifer.mcgrath@nhs.net
Vimal Vasu
Consultant Neonatologist, William Harvey Hospital, Ashford, Kent
Carol Sullivan
Consultant Neonatologist, Singleton Hospital, Swansea
On behalf of the BAPM Enhancing Shared Decision Making in Neonatal Care Working Group
Background
In November 2019, the British Association of Perinatal Medicine (BAPM) updated its existing 2004 document on consent as a framework on enhancing shared decision making in neonatal care.1 This framework reflects the increasing emphasis on the role of parents in neonatal care, the decline of medical paternalism in health care and the increasing emphasis of parental involvement in neonatal clinical decision making. More recently, the General Medical Council (GMC) has published an updated guidance on decision making and consent in health care, which came into effect in November 2020.2
Here, we provide a summary of the main areas in the BAPM framework, how it aligns with the new GMC guidance and some practical tips for how neonatal healthcare practitioners can translate guidance into clinical practice. Further details and how to put it all into practice are covered in the BAPM framework.1
The BAPM framework for practice
Over the past decade there has been a move away from paternalistic healthcare decision making towards one that incorporates working in partnership with parents when making decisions about a baby’s care. This family-centred ethos aligns with a parent’s moral and legal rights and with how the UK courts now consider the standard of information disclosure in health care post the landmark Supreme Court case of Montgomery v Lanarkshire Health Board (FIGURE 1).3 BAPM’s Enhancing Shared Decision Making in Neonatal Care – a Framework for Practice, codifies a number of principles of communication and shared decision making and provides a pragmatic and non-directive guide for all healthcare professionals involved in the care of babies to use in order to enhance shared decision making. It describes eight key principles (TABLE 1) that can be applied in day-to-day neonatal care to help enhance our involvement of parents in decision making along with some practical guidance on how to apply these principles.
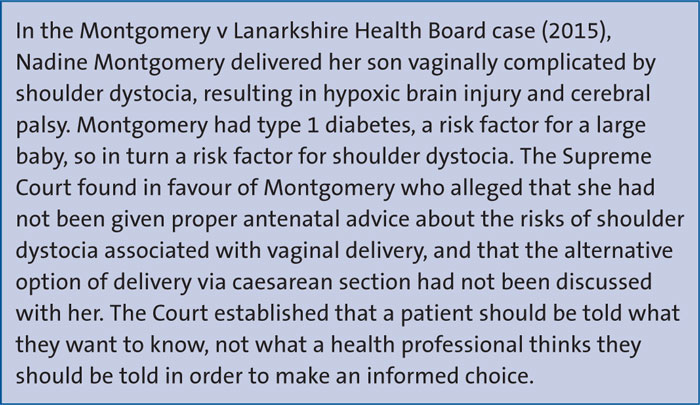
FIGURE 1 Montgomery v Lanarkshire Health Board.3
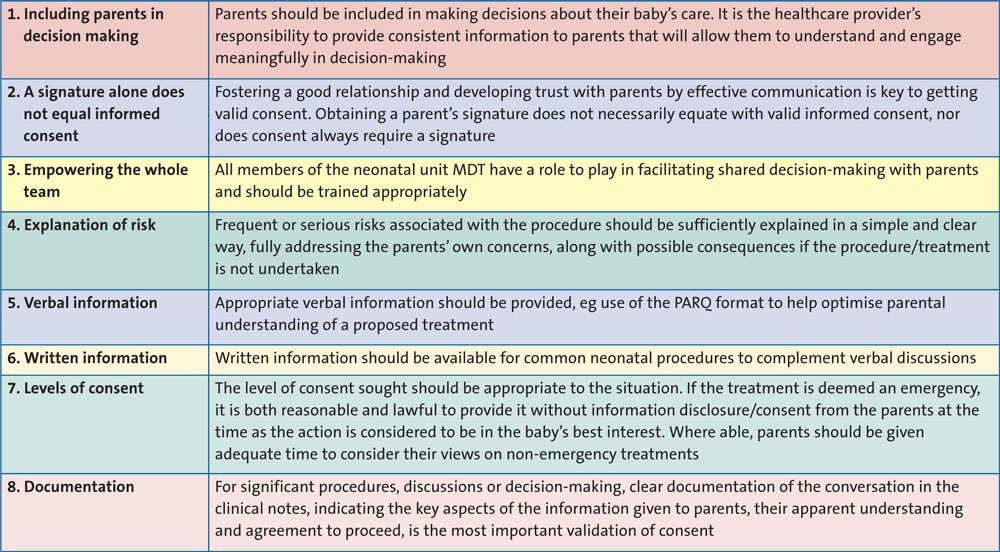
TABLE 1 BAPM: the eight principles of shared decision making.
Principle 1: Including parents in decision making
Where able to, healthcare professionals should aim to involve parents in decision making. Simply put, if there is time to do so, an intended procedure or intervention should be discussed. Neonatal care is often composed of a multitude of daily interventions with differing risk profiles and underlying evidence base. Consistency and clarity of information between different doctors and other healthcare professionals should take precedent over differing clinical views that may reflect professional biases. If there is clinical uncertainty over a proposed intervention, it should be acknowledged and the various options discussed. Developing systems that enable good multi-professional handover of information to parents and contemporaneous records of discussions with parents is encouraged.
As has been highlighted during the recent coronavirus pandemic, parents should not be considered as visitors and should be encouraged to be present, whenever possible, to deliver their baby’s care and be actively involved in decision making.4 Information sharing includes the principles shown in FIGURE 2.
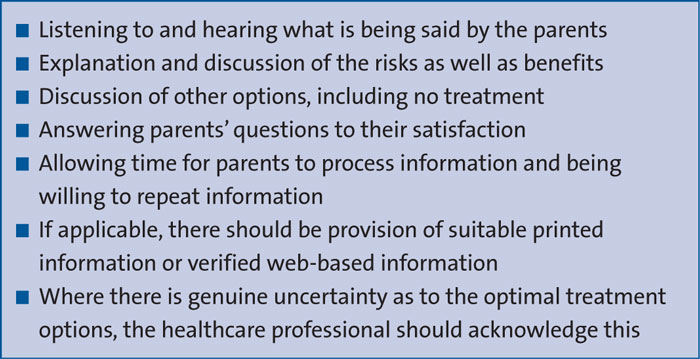
FIGURE 2 Information sharing principles.
Principle 2: A signature alone does not equal informed consent
In UK law, obtaining a signature does not equate with valid consent. There are several key principles for valid consent. The parent must have capacity to make an informed decision, the consent must be provided voluntarily (free from coercion by carers, family or friends) and the parent should be fully informed of the following with enough time allowed to reflect and ask questions:
- benefits and risks of the intended procedure
- alternative management strategies including doing nothing
- implications of not undergoing the proposed treatment.
Therefore, developing a strong, trusting relationship with parents is important as a tool to obtaining valid consent.
The use of non-medical terms, tailoring the information to what the parents want to know and what is materially important in terms of risks and benefits are key to shared decision making.
It is important to also consider the use of independent, approved translation services, so both parents receive an unbiased discussion, and other forms of advocates as appropriate to support communication.
Principle 3: Empowering the whole team
All members of the multidisciplinary team (MDT) have a role to play in facilitating shared decision making with parents. Some staff, such as nursing staff, can provide important continuity and useful insight. Appropriate and targeted training should be provided for the whole MDT to encourage and support communication, consistency of practice and to promote a family-centred approach to neonatal care. This training should be given on a regular basis and with evidence of engagement in such training reflected within the appraisal process.
Principle 4: Explanation of risk
Simple and sufficient explanations of frequent or serious risks associated with a procedure should be given, along with possible implications of not undertaking a specific treatment. Parents’ specific concerns should be addressed clearly and discussions tailored appropriately with an honest, frank and open dialogue. Parents can interpret risk in different ways and there are various methods for presenting risk to parents. It is important to remember some key principles:
- keep discussions about percentage risks simple
- understand the difference between positive and negative framing (eg 30% of failure versus 70% chance of success would represent negative and positive framing of the same outcome)
- ensure that if you are using numbers, denominators are kept consistent (eg rather than 1/5 risk of problem A and 3/10 risk of problem B, present as 2/10 and 3/10 risks for problems A and B, respectively)
- pictures and graphics may also be useful to explain risk.
Escalation via further discussions with more senior members of the team or duty of candour in line with the organisation’s policy should be undertaken if unexpected complications or notifiable safety incidents occur.
Principle 5: Verbal information
Verbal communication should be appropriate to the subject matter and audience. The acronym PARQ (procedure, alternative, risks, questions) can be helpful when discussing procedures with parents. Communication aids such as diagrams or infographics can be helpful. Parents should be empowered to be involved in decision making by using open-ended questions particularly when there is little evidence and/or several reasonable treatment options available.
Principle 6: Written information
Written information should be available for parents regarding common and low-risk procedures (such as cannulation) as well as medium- and higher-risk procedures. This should complement, not obviate, a verbal discussion about any procedure, regardless of the level of risk. Written discussion of risk should be in plain language, and translated versions available. The use of nationally available information for neonatal medical conditions, such as those provided by the charity BLISS,5 should be encouraged.
Principle 7: Levels of consent
The level of consent sought should be appropriate to the situation, be this emergency, semi-emergency or routine and should take into account the associated level of risk. Procedures can be divided into categories requiring implicit, explicit verbal or explicit written consent; this can be complex and is explored further in the framework with an appendix of examples. However as there is no robust evidence base for implicit or explicit verbal consent, these are examples of best practice to form a starting point for each neonatal unit or network’s discussion and guideline. Some units may prefer to seek consent for an integrated package of care (such as ‘special care package’ or ‘intensive care package’). All healthcare professionals should be aware of which procedures need which level or type of consent, as agreed by their unit.
If the treatment is deemed an emergency, it is both reasonable and lawful to provide it in the baby’s best interest, without discussion or consent from the parents. Where able, parents should be given adequate time and information to consider their views on non-emergency treatments. However for most procedures where there is a clear benefit-risk balance, consent should be mainly discussing plans with parents and seeking their consent, rather than asking them to make a decision about whether we should undertake a procedure.
An appendix is provided in the framework indicating who may hold parental responsibility in a range of scenarios.
Principle 8: Documentation
For significant procedures, discussions or decision making, clear documentation of the conversation in the clinical notes is the most important validation of consent. This should include the key aspects of the information given to parents, their apparent understanding and agreement to proceed, as well as who was present in the discussion.
It is considered acceptable that frequently performed day-to-day procedures, generally those of implicit consent, while still communicated to parents if they are present, do not usually need to have the discussion documented in the clinical notes as this is often not practical. This is a matter of judgement but if there is any doubt, it is recommended that the conversation is documented.
The 2020 GMC guidance
The GMC guidance, Decision Making and Consent,2 came into effect on 9 November 2020. It includes seven key principles that summarise the guidance (TABLE 2), plus a new section to help doctors find out what matters to patients in order to help them share relevant information for patients to decide between viable options. It also covers how other members of the healthcare team can support decision making.
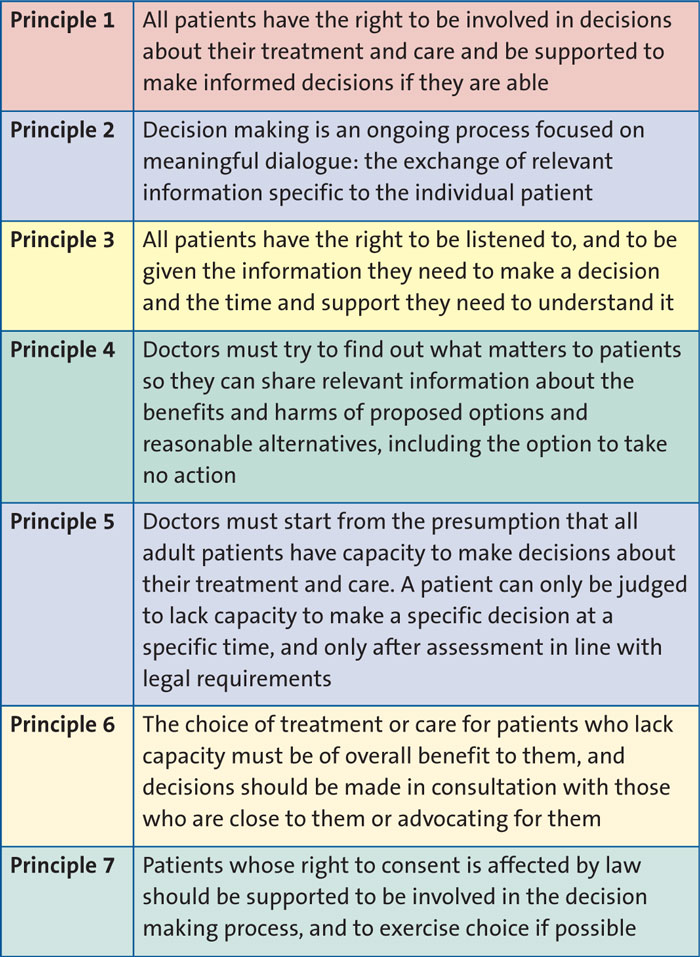
TABLE 2 GMC: The seven principles of decision making and consent.
The BAPM framework for practice and GMC guidance are complementary. In fact, replacing the word ‘patient’ in the GMC guidance with the word ‘family’ makes it easy to relate to neonatal care. The crux is that shared decision making and consent are fundamental to good medical practice. Getting this right can empower parents, which helps to improve health outcomes, patient experience and reduce complaints.
The aspects of GMC guidance on decision making and consent (2020) which are particularly relevant to neonatal care are shown in FIGURE 3.
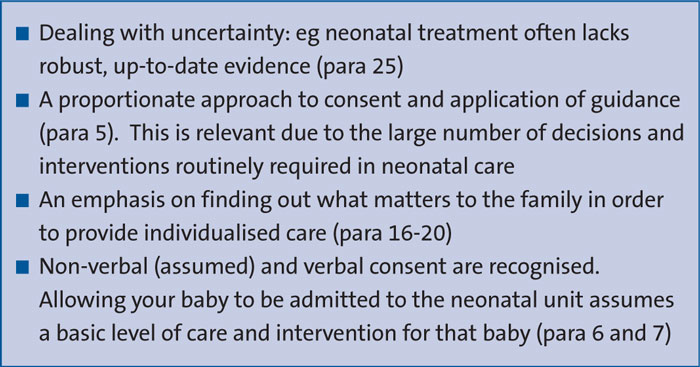
FIGURE 3 Aspects of GMC guidance on consent (2020)2 that are particularly relevant to neonatal care.
Other useful areas discussed in the BAPM framework for practice
How to proceed should parents not agree with a proposed procedure
The guiding principle of good medical practice is to make the care of the patient your first concern, which equates to a duty on all parties (professional and parental) to act in the baby’s best interests. It is rare for parents to disagree strongly when communication and information sharing are done well.
Predicting the possibility of conflict can allow early discussions prior to an emergency (eg with blood products and Jehovah’s Witnesses). Where disagreement does occur, it is often due to a misunderstanding, too much information or parents feeling pressured or anxious. Giving parents time to consider options (where this is feasible) and offering a second clinical opinion can often overcome such disagreements. If this is not successful, involvement of Trust legal services may be required for further advice but it is important that the clinical reasoning behind decisions is not lost during this escalation.
The GMC guidance makes reference to a useful factsheet which sets out some of the key legislation and case law relating to medical decision making and consent in the UK, although it is not intended to be a comprehensive list nor is it a substitute for independent, up-to-date legal advice. In addition, it clearly states that if you are not sure how the law applies in a given situation, you should seek advice through local procedures, consult your defence body or professional association, or seek independent legal advice.
Resources needed to deliver the BAPM framework for practice
The main resources needed to deliver the BAPM framework for practice are listed in FIGURE 4. Of particular importance is staff training. Suggestions to achieve this include:
- all neonatal units and networks should promote access to training courses for the whole MDT to help staff to develop their listening and communication skills, ensuring they under-stand the benefits of good communication and a family-centred approach to neonatal care. Training in communication should form part of the local induction for all clinical staff and be ongoing
- a list of available information leaflets and the local policy for gaining of consent for examination and treatment should be available to all staff
- trainee doctors and nurses should, with the parents’ agreement, attend discussions between senior staff and parents for training purposes
- parental feedback on the quality of information-sharing should be actively sought alongside routine feedback on care received.
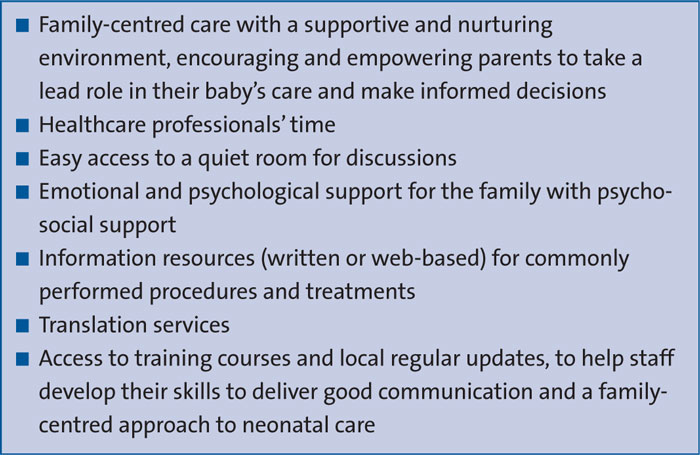
FIGURE 4 Resources needed to deliver the BAPM framework for practice.
How should the framework for practice and GMC guidance change my practice?
These guides should:
- re-emphasise the importance of parental involvement in decision making regarding the care of their baby
- encourage us to empower and train all members of the MDT to partake in information sharing with parents
- remind us of the difference between implicit and explicit consent with a signpost to examples of procedures and the level of consent they usually require
- provide a useful reference for guidance within the topic.
The guideline should also be used alongside GMC Good Medical Practice,6 GMC Ethical Guidance for Doctors 0-18 years,7 and Royal College of Nursing Principles of Consent: Guidance for Nursing Staff 2017.8
What does our team need to do now?
First of all, it is important that the whole team is aware of and reads the BAPM framework (note that the GMC guidance is addressed to doctors but still relevant to all). The BAPM framework touches on examples of the different types of consent.
It would be prudent to ensure a team discussion on how to approach consent for routine/frequently performed procedures and whether an integrated package of care and other decision making models would work for your unit.9 In addition, it is important to consider the inclusion of risk in patient information leaflets utilised in your unit.
Take-home messages
- Clear, open and consistent communication with families from the whole MDT is essential to engender a relationship of trust. This enables effective shared decision making.
- Valid consent does not always require a signature, nor does a signature equate to valid consent.
- The best interests of the baby should remain at the centre of all decisions of care by parents and professionals.
Acknowledgements
The authors would like to acknowledge Chelsie Letts from Bliss for her review and input into this article. The members of the BAPM working group are: Carol Sullivan, Singleton Hospital, Swansea (Chair); Dr Iyad Al-Muzaffar, Prince Charles Hospital, Merthyr Tydfil; Kate Dinwiddy, BAPM; Joanne Hodson, Royal United Hospital, Bath; Jennifer McGrath, St Peter’s Hospital, Chertsey, Surrey; David Millar, Royal Maternity Hospital, Belfast; Mary-Clare Ridge, Bliss; Vimal Vasu, William Harvey Hospital, Ashford, Kent.
Or read this article in our
Tablet/iPad edition
