

Congenital epulis and differential diagnoses of a neonatal oral mass
Oral mass in a newborn is rare but often quite daunting, leading to anxiety in parents. Very few hospitals have dental or maxillofacial facilities on site and this may lead to delayed diagnosis and intervention. A thorough clinical examination and knowledge of the oral mass is essential for precise diagnosis, management and parental reassurance. In this review article, we present a newborn baby with congenital epulis – an oral mass arising from the alveolar ridge. We also summarise the differential diagnoses based on location and consistency of the oral masses in this age group.
Anoop PahujaConsultant Neonatologist
anoop.pahuja@nhs.net
Harry James
ST3 Neonatology
Walton D’Costa
Consultant Neonatologist
Ghaida Al-Jaddir
Senior Consultant/Specialist in Paediatric Dentistry
Dilpreet Kaur
Consultant Paediatrician
Chelsea and Westminster NHS Foundation Trust
The case
A baby girl was born at term with a birth weight of 3.3kg. She was born to a primigravida with an uneventful pregnancy, normal serology and normal antenatal anomaly scans. The last scan was performed at 20 weeks of pregnancy. The mother had a history of Hodgkin lymphoma and had received radiotherapy and chemotherapy almost a decade previously. The baby was born by assisted vaginal delivery with Apgar scores of 9 and 9 at one and five minutes, respectively. The baby was breastfed and she was latching well and sucking without any difficulty.
A swelling over the lower gum was noted by a midwife on the initial check and the neonatal team was called to review. The swelling was round, solitary, 2x2cm in size and arising from the lower alveolar ridge over future canines (FIGURE 1). The swelling was firm in consistency with a smooth surface and non-tender on palpation. The parents were understandably anxious, especially due to the family history of lymphoma. She was reviewed by the dental team and the diagnosis of congenital epulis was confirmed.

FIGURE 1 Congenital epulis arising from the lower alveolar ridge.
The plan was for conservative management. The child would be actively monitored for change with regular review of the size/shape of the epulis, evidence of bleeding or pain, difficulty in feeding or breathing, weight gain and dentition. The management plan was explained to the parents and they were reassured about the benign nature of the mass and likelihood of self-resolution.
Discussion
Congenital epulis of the newborn
Congenital epulides are benign mesenchymal tumours arising from the anterior alveolar ridge, composed of large cells with a coarse granular cytoplasm. They were first described by Neumann in 1871 and later explained by Zuker and Buenecha1 in 1993. They are usually present at birth or appear soon after. Growth generally starts antenatally around the 22nd week of gestation, hence they are unlikely to be diagnosed on anomaly scans performed between 12 to 20 weeks.2 Large lesions may be picked on late antenatal scans and MRI is the preferred modality to assess the extent of the lesion and help plan delivery.
They appear as smooth, non-ulcerated polypoid masses with a broad-based attachment to the alveolar ridge, with preference for the maxilla over the mandible and overlying the future canine and lateral incisor teeth. Although usually singular, about 10% of reported cases are multiple or a cluster of small tumours with potential to cause mechanical obstruction, respiratory and feeding difficulties.3
Congenital epulides are rare with an incidence of 0.0006%.4-6 Females are affected more often than males (9:1).7 Various aetiologies are proposed including odontogenic, neurogenic, myoblastic, endocrinologic, fibroblastic or histiocytic origin.8,9 Female predominance may favour the endocrine theory of aetiology.
Epulides are usually benign, but the obstructive masses may cause difficulty with respiration and feeding. They stop growing at birth and often regress over time. Local conservative resection, under local anaesthesia for small epulides, is curative and only required if causing difficulty in feeding or breathing. Surgical excision is required if affecting the growth of the bone or the eruption of teeth. Even after incomplete excision, they do not recur.10-12
Oral masses in the newborn period
A wide range of diseases present as oral lesions in the newborn period; fortunately, the majority are benign. A thorough clinical examination and knowledge of the oral mass is essential for precise diagnosis and management. Oral lesions in neonates include:
- cysts
- infections
- traumatic lesions
- tumours
- autoimmune diseases.
Malignant tumours of soft tissue, salivary glands and bones must be considered.
The list of conditions to consider in the differential diagnosis for a congenital oral mass is long but identification based on anatomical location in the oral cavity (TABLE 1) and consistency (FIGURE 2) helps to narrow the diagnosis.
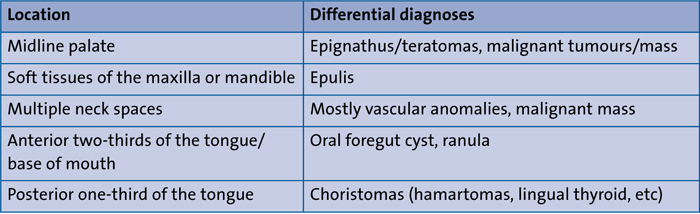
TABLE 1 Differential diagnoses for an oral mass based on anatomical location in the oral cavity.13
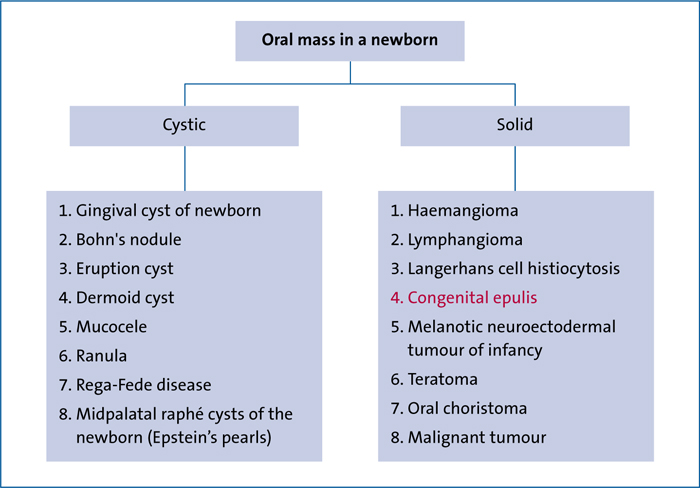
FIGURE 2 Differential diagnoses for an oral mass based on consistency.
Cystic oral masses (TABLE 2)
Gingival cyst of the newborn
Also known as dental lamina cyst. A small, benign oral mucosal lesion, usually multiple and nodular. White to cream-coloured lesions.14-17
Bohn's nodule
A keratin-filled nodular cyst that presents as small, whitish lesions that do not increase in size. When present on the anterior mandibular ridge they may be misdiagnosed as natal teeth.15-18
Eruption cyst
Presents as a bluish, dome-shaped, translucent, compressible swelling within the mucosa, overlying an erupting tooth.15,19
Dermoid and epidermoid cysts
Rare benign, asymptomatic and slow-growing cysts. Diagnosed if/when enlarged with a potential risk of respiratory distress and feeding difficulty.16,17,19
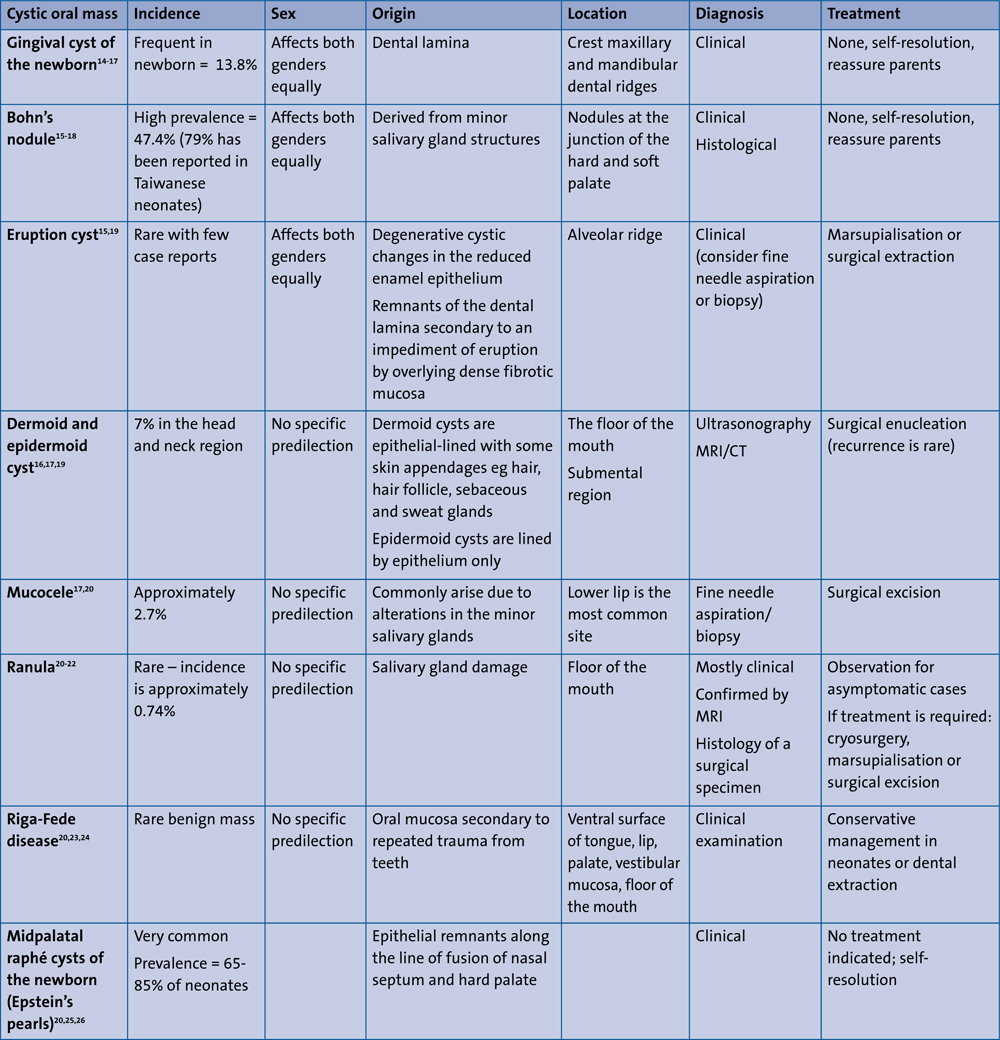
TABLE 2 Cystic oral mass in the newborn period – differential diagnoses.
Mucocele
Presents as a bluish (depending on the proximity to the surface), translucent and fluctuant swelling that may cause mechanical obstruction during feeding.17,20
Ranula
A painless swelling in the floor of the mouth commonly caused by extravasation of mucin.20-22
Rega-Fede disease
Appears as an ulcerated/cystic or fibrous mucosal mass. The neonatal type is benign and commonly associated with natal/neonatal teeth. Unifocal/multifocal and occasionally painful.20,23,24
Midpalatal raphé cysts of the newborn (Epstein’s pearls)
Small (1-3mm) yellow-white papules along the midpalatal raphé, especially at the junction of the hard and soft palate. The cysts are filled with keratin.20,25,26
Solid oral masses (TABLE 3)
Haemangioma
The most common vascular benign mass. Manifests as a rapidly growing macule followed by regression into spotted pigments.27,28 Can be present at birth but tends to develop a few weeks after birth. There are three phases of development:
- rapid proliferating phase (0-1 year)
- involuting phase (1-5 years)
- involuted phase (5-10 years).
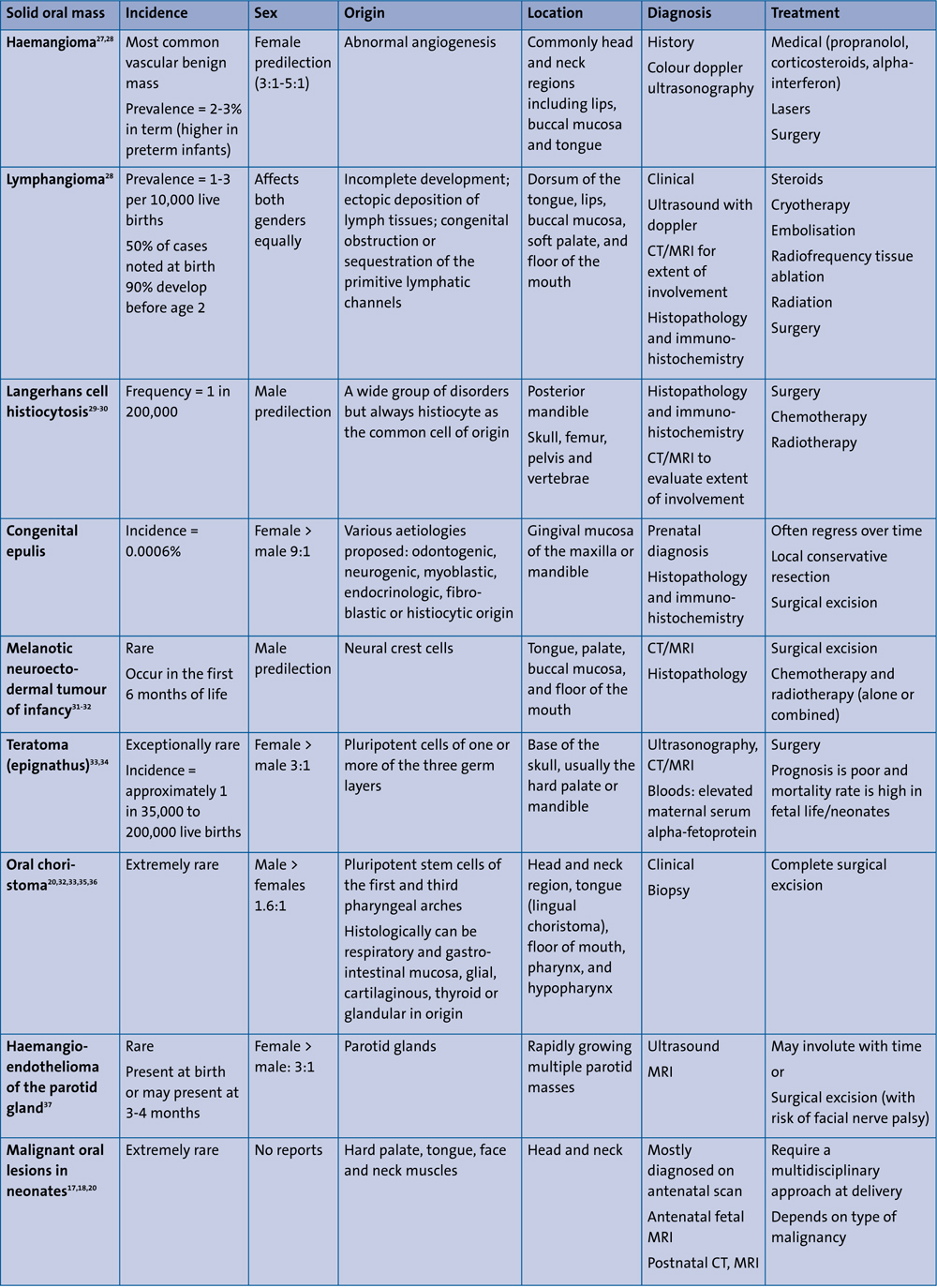
TABLE 3 Solid oral mass in the newborn period – differential diagnoses.
Lymphangioma
Benign congenital tumours of the lymphatic system. Oral lesions present with macroglossia, dysphagia, ulcerations, deformity of jaws, and feeding problems. A lymphangioma can be superficial (slow, progressive lesion with superficial blue-black or red haemorrhagic elevated nodules), deep (soft, diffuse growths with normal colour) or cystic (soft, painless fluid-filled lesions, characteristically located in the neck).28
Langerhans cell histiocytosis
Congenital self-healing reticulohistio-cytosis presenting at birth and showing complete involution within 2-3 months. Characteristic features include; erythematous vesicular-pustules with/without crusting and eczematous scaling of the skin; oral petechiae, swelling of the gingiva; X-ray lytic lesions. Depending on severity and extent, systemic findings may include hepatomegaly, splenomegaly, pancytopenia, and central nervous system involvement.29,30
Melanotic neuroectodermal tumour of infancy
Characterised by benign, painless, non-ulcerative, expansile, rapidly growing, pigmented lesions.31-32
Teratoma
Presents as an oral mass with mass effect – eg poor feeding, breathing difficulty. May have an intracranial component.33,34
Oral choristoma
Abnormal location of histologically normal tissue. Mostly asymptomatic but with space-occupying effects. Can be cystic or solid depending on the tissue of origin.20,32,33,35,36
Malignant tumour
A solid space-occupying lesion mostly diagnosed on antenatal scans. The mass may interfere with feeding and respiration, depending on location. For example, malignant melanoma of palate and spindle cell sarcoma of tongue.17,18,20
Patient consent
The authors received written consent to publish this report from the patient’s parents.
Or read this article in our
Tablet/iPad edition
- Congenital epulis is an uncommon benign swelling present on the gingivae of newborn infants.
- Epulis can be confused with many other diseases that present as oral lesions in the newborn period.
- Distinguishing and diagnosing oral masses in the newborn period is discussed.
