

Persistent left superior vena cava and the correct interpretation of a peripherally inserted central catheter tip position
This article reports on a case of a preterm baby who, post-routine insertion of a peripherally inserted central catheter (PICC), showed an unusual catheter route and tip placement revealing an unsuspected cardiac variant of persistent left superior vena cava (PLSVC). We discuss the condition, our management and its effects on vascular access in this unusual case.
Matheus van Rens1Director of Nursing and Vascular Access, NICU
mrens@hamad.qa
Kevin Hugill2
Director of Nursing (Education)
Aala Eldin Fawzy Mohamed El Fakharany1
Consultant Radiologist, Clinical Imaging Department
Krisha Leigh Garcia1
Nurse Educator, NICU
1Women’s Wellness and Research Center, Hamad Medical Corporation, Doha, Qatar
2Nursing and Midwifery Education Department, Hamad Medical Corporation, Doha, Qatar
The case
A preterm male baby was born at 29 weeks and 5 days by emergency caesarean section to non-consanguineous parents for severe maternal pre-eclampsia. The mother was a 36-year-old woman of gravida 4, para 3 who presented with gestational diabetes and a history of placenta previa with her previous preg-nancy. The infant was born in good condition and did not require resuscitation. At birth, his Apgar scores were 7 and 9 at one and five minutes, respectively. His birth weight was 1,170g and he had a head circumference of 25.5cm. Physical examination revealed bilateral congenital talipes equinovarus but nothing else of note.
On admission to the neonatal intensive care unit (NICU) all his vital signs were stable and within normal/expected ranges. He received short-term respiratory support (continuous positive airway pressure) and one dose of surfactant using the less invasive surfactant administration (LISA) technique for respiratory distress syndrome. Due to prematurity the need for long-term (>5 days) vascular access was indicated. As per local practice, an initial peripheral IV catheter was inserted, and the baby was scheduled for a PICC insertion on day two of life.
PICC insertion process
After obtaining informed consent from the parents, a dedicated PICC team trained for PICC insertion performed the actual insertion.1 As planned, the insertion took place on day two of life using the modified Seldinger technique (MST) with a prepared Premistar (Vygon) 20cm PICC as per local evidence-based guideline.2-4 After a standardised mandatory vascular assess-ment, the left cephalic vein was identified as the insertion vein of choice. A pre-measured length of 18cm was determined to enable the PICC tip to be as close as possible to the right atrium but remain outside the heart. The PICC insertion procedure itself was straightforward and seemingly successful, however, there was notably more bleeding at the site than was usual.
Anatomically the PICC should reside inside the superior vena cava and be seen on the right side of the vertebrae/spinal column. A review of the post-procedure X-ray (FIGURE 1) showed a descending PICC on the left side of the vertebrae/spinal column. Based on this observation, a concern was raised as to the exact catheter placement. The radiologist’s report described: “Left upper limb PICC line appears malpositioned overlying cardiac shadow.” In view of this finding and based on the adage, ‘if in doubt, take it out’, the catheter was removed. A second PICC was inserted without incident into a different vein.
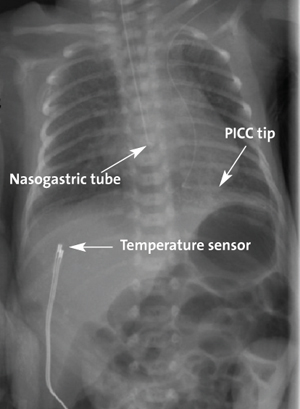
FIGURE 1 The misplaced PICC visualised by X-ray on the left side of the vertebrae. The nasogastric tube and PICC were repositioned after review of the X-ray.
Discussion
Initial suspicions
During post-procedure debriefing, it was speculated that the PICC might have been accidentally inserted through the brachial artery, advancing through the subclavian artery and aorta with the tip residing in the left cardiac ventricle. The unusual bleeding seen during the insertion procedure was cited in support of this doubt. However, it was considered highly unlikely that the brachial artery was inadvertently cannulated. We routinely use a vascular visualisation device (VeinViewer, Christy Medical Corporation) as a part of pre-procedural site selection. With this device, clinicians can see peripheral veins, bifurcations and valves, and assess in real time the refill/flushing of veins and be confident they are accessing a vein. The infrared technology used by the device only provides information from desaturated blood, hence under normal circumstances only veins are projected. In this case the left cephalic vein was clearly visualised pre-procedure and during the entirety of the procedure itself.
While bleeding from the puncture site was more than usual (clotting was normal) the colour of the blood was a darker shade of red and not the typical hue of arterial.5 Furthermore, tissue bleeding caused by an arterial puncture would have been observable by the projected image of VeinViewer as a ‘blur’. This situation would have made it difficult to further visualise the insertion site. Consequently, the speculation that practitioners had inadvertently accessed the wrong blood vessel (brachial artery) was discounted. Nevertheless, the evident malposition of the PICC required explanation.
PLSVC
The route the PICC followed was abnormal. One possibility was that the PICC had deviated from the left upper extremity veins into the left-sided paraspinal hemiazygos venous system.6 However, clinical and radiologist consensus was that a PLSVC (FIGURE 2) was the most likely explanation for the PICC’s route.
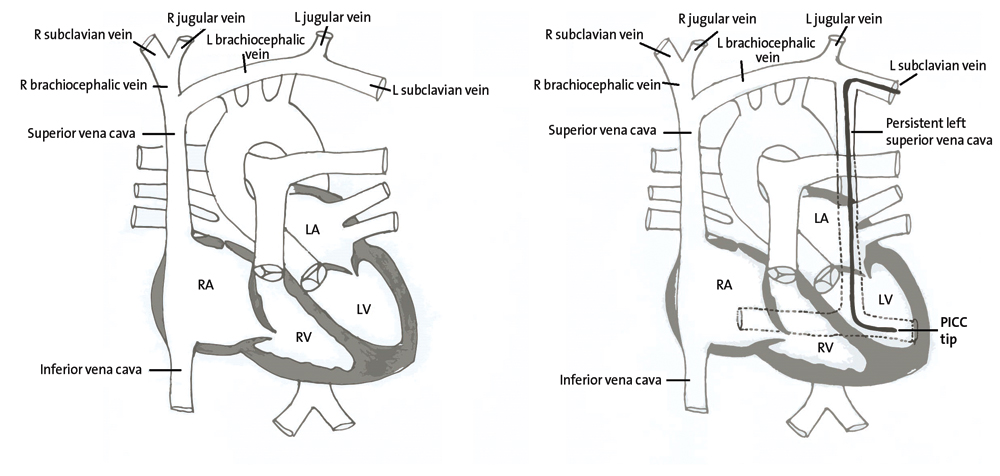
FIGURE 2 Anatomy of the heart: normal (left) compared with PLSVC (right), showing the route of the PICC due to abnormal venous anatomy. Key: RA=right atrium; LA=left atrium; LV=left ventricle; RV=right ventricle.
PLSVC is a known vascular variant, although reports of its incidence vary.
In a recent study Chao et al reported an incidence of 0.29% in a population of healthy neonates.7 Others have observed rates of 0.5-2% among the general population8 and 0.7-0.9% in fetuses.9-12
The aetiology of the condition relates to a failure of early blood vessels to regress during embryonic development specifically, the right and left anterior cardinal veins. These vessels constitute the main venous drainage of the cephalic portion of the embryo. Normally, at around eight weeks of development the left anterior cardinal vein regresses (later becoming the ligament of Marshall); if this fails to happen, it leads to PLSVC.7,13,14 Most often, when a PLSVC is present, a normal right superior cava is also present, though there is considerable variation in venous architecture.14,15
Isolated PLSVC is usually asymptomatic with few clinical features and is often detected as an incidental finding during other medical and surgical procedures (sometimes in adulthood).12,14-16 The importance of PLSVC in neonatal care settings lies in a greater association with chromosomal congenital heart defects8,10,12 and how it impacts upon central line placement when using the left arm. Therefore, the recognition of a PLSVC should alert healthcare professionals to these risks and the need for appropriate investigations (eg echocardiography).9
PICC insertions in neonates are considered safe and success rates of insertions are relatively high.3-4 PICC insertion and ensuring correct tip positioning can be challenging in babies with abnormal venous anatomy. Misplaced catheters are a cause of concern due to them posing an increased risk of complications and adverse clinical events, which can be fatal. It is common that malpositioned catheters will either be removed (or repositioned to a midline position) to avoid these risks. Opinion, with the benefit of hindsight and more information about whether the catheter should have been removed (as was the case) or retained in situ prior to further diagnostic investigations, differed. However, based on the information available at the time and on the principle of patient safety first, we believe that early removal was the safest course of action.
Afterword
After the initial ‘failed’ insertion a second PICC was inserted and by day 13 of life IV therapy was completed and the PICC successfully removed. The baby developed an IVH Grade II on day 6 of life but currently the baby is well and at home. Post-discharge management involves physiotherapy and orthopaedic management of the congenital talipes equinovarus and multi-professional developmental and cardiology follow up.
A further note needs to be made related to the congenital talipes equinovarus in relation to a potential PLSVC. While congenital talipes equinovarus may occur as an isolated birth defect with no other malformations (80% of cases), it also can be secondary or syndromic when its presentation is associated with another congenital disease (20% of cases).13 In our case, aside from the PLSVC, we have found no other features to suggest a link between these two anomalies.
Conclusion
The case reported here of an infant with a PICC tip residing in a PLSVC posed local debate about the best course of action to take. Nevertheless, this experience has raised awareness of the need for practitioners to be aware of the potential for unusual features like PLSVC, to confound our practice expectations and prompted exploration of whether to adopt newer technologies (such as bedside ultrasound) into our PICC insertion practice portfolio.
Permissions and acknowledgements
This case report and its publication was approved by the local Institutional Review Board (MRC-04-20-629), as is the norm in this setting. As the case study has no identifiers, a written informed consent for publication of the case history was not requested.
The authors are grateful to Kayce Leinne Garcia for the illustrations and Goutham Babu for review of the initial draft.
Or read this article in our
Tablet/iPad edition
- PLSVC is a rare cardiac venous anatomical variant that is usually encountered by chance.
- Examination of PICC tip position and its vascular route confirms correct PICC placement. Practitioners should be aware that unusual anatomical variations in venous architecture can complicate PICC placement and tip position interpretation.
