

Perinatal asphyxia: don’t forget the placenta
This report highlights the importance of examination of the placenta in neonates with evidence of perinatal asphyxia, even when history may suggest a sentinel event.
Tayyaba Yasmeen1ST5 Paediatrics
tayyaba.yasmeen@ggc.scot.nhs.uk
Cara Owens1
Specialty Doctor, Paediatrics
Althaf Ansary1
Neonatal Consultant
Sheena Kinmond1
Neonatal Consultant
Jane Ramsay2
Obstetric Consultant
Paul French3
Consultant Paediatric Pathologist
1Neonatal Unit, Ayrshire Maternity Unit, Crosshouse, Kilmarnock;
2Obstetrics and Gynaecology, University Hospital Crosshouse, Kilmarnock;
3Pathology, Queen Elizabeth University Hospital, Glasgow
Case report
A boy was delivered at 37 weeks’ gestation by emergency caesarean section for fetal bradycardia following a small antepartum haemorrhage; there had been a spontaneous rupture of membranes the previous day. Until then, the pregnancy had been uneventful.
The infant had no detectable heart rate until 21 minutes into full resuscitation according to Resuscitation Council guidelines. He had abnormal neurological findings and went on to develop seizures; the initial amplitude-integrated EEG (aEEG) showed burst suppression. He also developed multi-organ dysfunction. He was cooled for 72 hours and subsequently made a good clinical recovery, being discharged on day 28 of life, fully enterally fed, seizure-free and off anti-epileptics. Magnetic resonance imaging (MRI) on day 16 showed cystic changes in the periventricular white matter adjacent to the anterior horns/ventricular bodies bilaterally, in keeping with a global hypoxic insult.
Placental histology showed:
- velamentous cord insertion (VCI) with no trauma to blood vessels
- delayed villous maturation (DVM).
DVM was the most likely underlying explanation for his perinatal asphyxia.
A brief revision lesson in physiology
The placenta facilitates the roles of gas, nutrient and waste exchange as well as secreting hormones important to both mother and baby (FIGURE 1). It develops over the course of a pregnancy to reflect dynamic adaptation to oxygen and nutrition demands during pregnancy. Over time, chorionic villi increase in size and branch to accommodate the increased demand of the developing fetus. During the first and second trimester, the villi are predom-inantly immature, intermediate villi; in the third trimester, mature intermediate and terminal villi are seen.
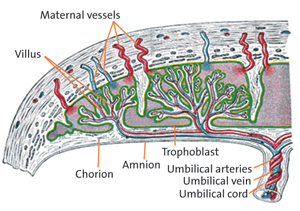
FIGURE 1 Anatomy of the placenta.
Terminal villi, the final branches of the villous tree, present a large surface area richly vascularised by fetal capillary networks with sinusoids, which bring endothelium into close approximation to the covering of trophoblasts. These are called vasculosyncytial membranes and are the principal sites of maternal-fetal exchange. Oxygen moves by diffusion. An increase of two-fold in the distance between blood supplies decreases the fetal oxygen concentration four-fold.
VCI
A VCI is an abnormal cord insertion where the umbilical vessels diverge as they traverse between the amnion and chorion before reaching the placenta (FIGURE 2). These vessels lack protection from Wharton’s jelly and can easily be compressed resulting in rupture, especially during labour. Perinatal death at term increases three-fold with VCI, although this is an unlikely cause of hypoxic-ischaemic encephalopathy (HIE) in this case, as the mother was not in labour.
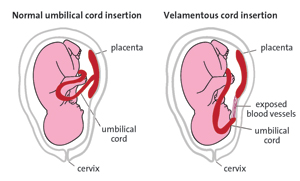
FIGURE 2 Velamentous cord insertion. The umbilical cord attaches to the membranes surrounding the placenta rather than the central placental mass, leaving umbilical vessels unprotected.
DVM
The persistence of immature intermediate villi with a thickened layer of trophoblasts results in very few vasculosyncytial membranes, which impairs gas exchange (FIGURE 3). DVM can be caused by:
- excessive placental growth factor
- excessive vascular remodelling
- dysregulation of developmental placental gene expression.
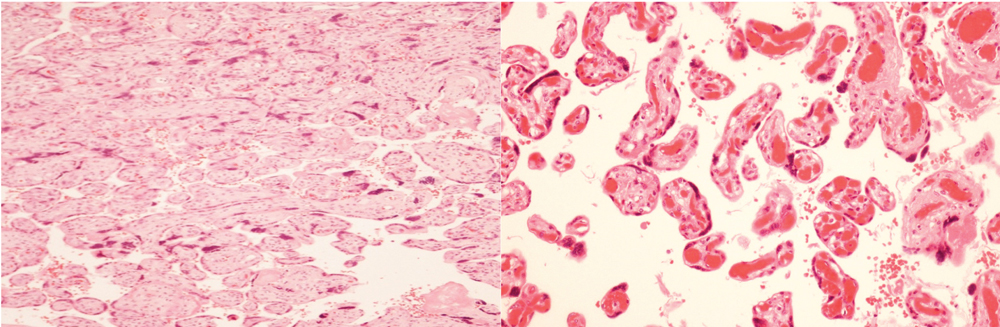
FIGURE 3 Placental histology. Left: Very few vasculosyncytial membranes in terminal villi, in keeping with delayed villous maturation. Right: Control sample showing vasculosyncytial membranes.
It results in inefficient nutrient and gas exchange meaning that the fetus is less able to withstand any stressors or periods of increased demand/hypoxia, such as labour or antepartum haemorrhage. The delayed maturation occurs at around 34-35 weeks of pregnancy and therefore cannot be predicted any earlier. The outcome is often a late intrauterine death with some studies suggesting a 70-times higher risk than with a normal placenta. There is a high risk of reoccurrence in subsequent pregnancies.
Conclusion/learning points
- The underlying aetiology of HIE may not be fully recognised, whether or not there has been an obvious sentinel event that appears to explain the infant’s condition.
- Placental examination and histology more often provide additional information on the likely cause of HIE.
- Neonatologists should remember that placental pathology can be vital in understanding the aetiology in such cases.
- Findings may well be incidental and the case history should always be reviewed along with histology.
Or read this article in our
Tablet/iPad edition
