

Optimising early maternal breast milk for preterm babies: a quality improvement toolkit
The British Association of Perinatal Medicine (BAPM) and the National Neonatal Audit Programme (NNAP) are collaborating on four quality improvement toolkits to support perinatal staff to implement the evidence around perinatal optimisation. This article presents the Maternal Breast Milk Toolkit. The key focus of this toolkit is to support the optimisation of early maternal breast milk to improve the proportion of preterm babies receiving their mother’s own milk.
Sarah BatesConsultant Paediatrician and Neonatologist, Great Western Hospitals NHS Foundation Trust, BAPM Executive Committee
Gillian Bowker
Infant Feeding Advisor, NHS Greater Glasgow and Clyde
Sara Clarke
Senior Specialist, Neonatal Network Dietitian, West Midlands Neonatal ODN
On behalf of the BAPM MBM Toolkit Group
Maternal breast milk (MBM) provides the optimal form of feeding for preterm infants (FIGURE 1). Specific health benefits for the preterm infant population include lower mortality rates, lower rates of sepsis and necrotising enterocolitis,1,2 improved neurodevelopmental outcomes,3 lower rates of bronchopulmonary dysplasia4 and retinopathy of prematurity,5 and fewer hospitalisations in the first year after discharge compared to formula feeding.6 The World Health Organization7 and specialty consensus guidelines across multiple areas of neonatology8-10 recommend maximising the use of MBM for premature and sick babies. Mothers of vulnerable infants, such as extremely premature infants, encounter a variety of unique breastfeeding barriers and challenges. Despite the known benefits of maximising MBM for very preterm babies, a large proportion of preterm babies in the UK are not fed an exclusive breast milk diet. Indeed the 2019 NNAP11 reports only 55% of very preterm infants are fed with some of their mother’s own milk at discharge and this figure has remained persistently low over the last five years. NNAP recommendations focus on not only the main-tenance of lactation, with the attainment of preterm infants receiving their mother’s own milk at discharge, but on the early initiation of breast milk expression and administration to infants.
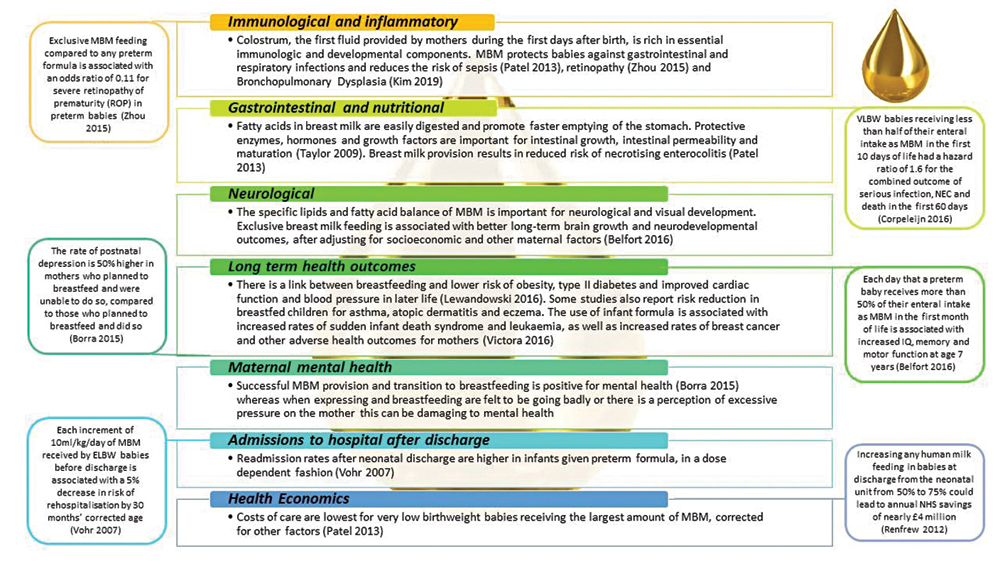
FIGURE 1 The impact of MBM on preterm babies.1-6,12-16 Key: MBM=maternal breast milk, VLBW=very low birth weight, ELBW=extremely low birth weight, NEC=necrotising enterocolitis.
What is the context for the toolkit?
BAPM aims to improve standards of perinatal care by supporting all those involved in providing this care to optimise their skills and knowledge. A key value of BAPM is ‘working collaboratively’ to provide the safest and most effective service for babies and this toolkit has been developed by a multidisciplinary team (MDT) of neonatal health professionals.
With these shared goals in mind, BAPM, NNAP and other key stakeholder organisations in perinatal care are collaborating in a three-year national quality improvement (QI) initiative that will target key NNAP measures and aligns with and supports other neonatal national workstreams. Improvement at local and national level will be measured by NNAP.
The Perinatal Optimisation Care Pathway
Perinatal optimisation refers to the process of reliably delivering evidence-based interventions in the antenatal, intrapartum and neonatal period to improve preterm outcomes. The BAPM Perinatal Optimisation Care Pathway (FIGURE 2) refers to these interventions as they occur temporally, and applies to both the mother and her baby. The pathway is supported by four BAPM toolkits (Antenatal Optimisation, Optimal Cord Management, Normothermia and Maternal Breast Milk).
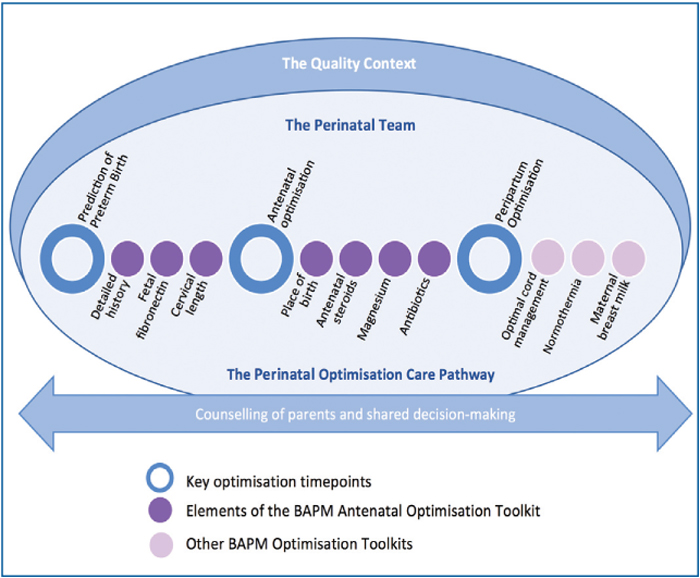
FIGURE 2 The Perinatal Optimisation Care Pathway.
This Perinatal Optimisation Pathway sits within the remit of the local and network ‘perinatal team’ whose strong team-working culture, high quality communication habits and pursuit of common goals result in the reliable delivery of these interventions. Such implementation success can only occur within a suitable context where structure and processes support an optimal environment for QI. Such key contextual features are described in the BAPM Neonatal Service Quality Indicators.17
How will this toolkit help me implement the use of early MBM?
Providing MBM for mothers of preterm babies depends on a complex system of multidisciplinary and holistic interventions that focus on individual, structural, cultural and environmental factors. The key focus of this toolkit is supporting the implemen-tation of the five perinatal core elements to optimise early MBM for preterm babies (TABLE 1) in order to improve the proportion of preterm babies receiving their mother’s own milk by:
- providing the evidence for effective interventions, including examples of what is proven to work in improving MBM for preterm babies
- facilitating individual units to interrogate their data and processes in order to undertake pertinent selected QI and sustain momentum
- providing easy to use QI tools and assisting units to interpret and monitor results of their QI activity
- signposting existing resources for optimising MBM for adaptation for local use.
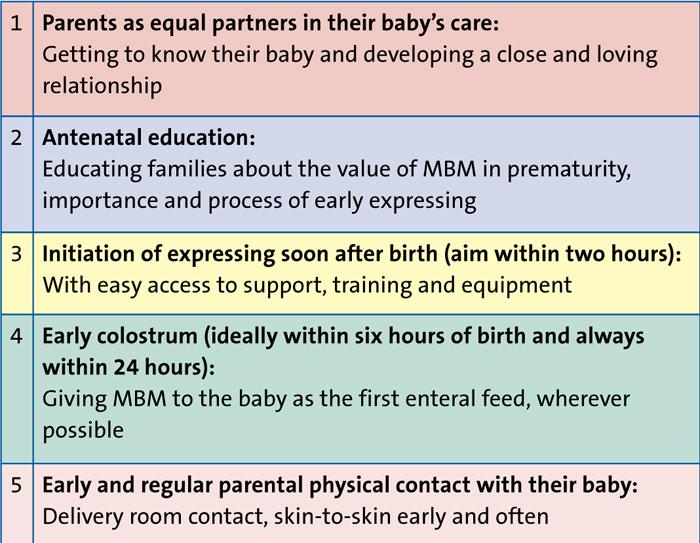
TABLE 1 The five perinatal core elements for supporting optimisation of early MBM.
The five perinatal core elements
The first key step to the establishment of a good maternal milk supply lies in the perinatal period. The volumes of milk mothers can express as early as day 3 or 4 of life are highly correlated with long-term breastfeeding outcomes,18-20 supporting the idea that this early period is a critical window. There are a number of strategies to increase early MBM delivery to very preterm babies with the evidence base ranging from moderate quality to best practice, including consensus expert opinion. Each of the five perinatal core elements has a summary of the most relevant or useful evidence to support its implementation.
1. Parents as equal partners in their baby’s care
Family-centred and family-integrated care (FIC) starts in the perinatal period to ensure that parents are central to their baby’s care even when the baby is born preterm or sick.21,22 While there is limited evidence linking the use of FIC with provision of early MBM, there are many studies showing a positive effect of FIC and parental involvement on breastfeeding at discharge.23-25
2. Antenatal education
Educating families about MBM is essential for those mothers identified early in pregnancy as being at increased risk of preterm birth. More targeted time-critical education is important for families where preterm birth is imminent.
Lactation-specific antenatal counselling increases exclusive breastfeeding at discharge and studies show that mothers who had planned to formula feed identified positive consequences of initiating breast milk expression.25-27 Lactation counselling should cover:
- the specific benefit of MBM for the preterm baby
- the vital importance of starting to express as soon as possible after birth
- realistic volumes of colostrum expected
- familiarisation with the techniques and equipment involved.
The focus of discussions should not be on the long-term benefits of breastfeeding, but on the unique protective benefits of colostrum and breast milk for the preterm infant during their time in the neonatal unit.
3. Initiation of expressing soon after birth
Facilitating expressing soon after birth (aim = within two hours) requires a multidisciplinary, collaborative approach between the midwifery staff, obstetricians and neonatal staff to provide sensitive support and education to the mother at this key time. Central to the planning for preterm delivery should be a discussion with parents about the benefits of early expressing. Evidence points to early initiation of expressing increasing yields of MBM and increased MBM feeding at discharge.28,29 For many parents, the first few hours after birth of a sick or preterm baby can be very stressful. This is especially true where they are separated from their baby or the mother is unwell. Sensitive conversations and effective, timely support can empower women to initiate their lactation even in difficult circumstances (FIGURE 3). Many women who are ill themselves wish to initiate expressing and illness alone should not preclude conversations taking place and support for expressing being given.
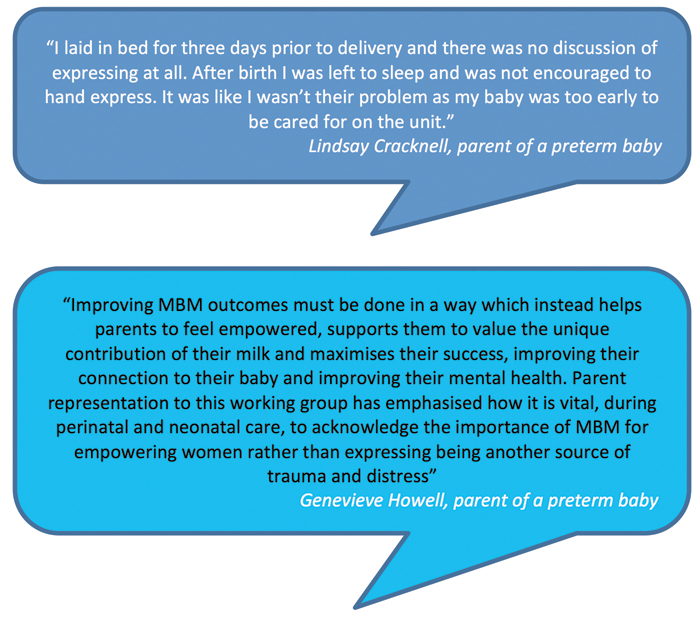
FIGURE 3 The importance of effective, timely support and empowering women to initiate lactation.
Information and support with technique and frequency of expressing in the early days will maximise lactation. Reinforcing the benefits of very small volumes of colostrum will encourage and empower the woman. In the early days the focus should be on perfecting techniques to support effective hand expressing and breast pump use. This should include the importance of breast massage and relaxation linking it to hormonal responses and milk supply. Ensuring that parents have a realistic understanding of likely colostrum volumes in the post-partum period will prevent distress and discouragement. Volume-driven expressing should be avoided at this stage, but a focus on the process of attempting to express will provide valuable stimulation to the breast tissue and hormone pathways to initiate milk supply.
4. Early colostrum
Early administration of colostrum (ideally within six hours of birth and always within 24 hours) is reported in the literature as:
- supporting immune responses30
- reducing time to full feeds31
- reducing the incidence of ventilator-associated pneumonia32
- associated with increased MBM feeding at six weeks and at discharge.33
The provision of early colostrum to a baby is dependent on getting expressed colostrum to the neonatal unit and administered to the baby. Consideration should be given to the whole process from antenatal conversations right through to administration of buccal colostrum. Identification of barriers and enablers at each stage of the process will identify where additional work may be required. To maximise success, colostrum and early breast milk must be valued and prioritised by all members of the MDT. Neonatal teams should prioritise giving colostrum as the first feed.
5. Early and regular physical contact
This intervention is based on the prioritisation of physical contact between parents and their baby from the earliest time point following birth and onwards, while maintaining optimal respiratory and thermal support. Training to ensure staff confidence and skills in maintaining baby safety and stability in the transfer to skin-to-skin care is essential. Evidence supports early and prolonged skin-to-skin contact as it improves expressed MBM volumes, and breast milk feeding rates at discharge.34-36
An overview of the improvement journey
How to start?
Beginning any QI work can be a daunting task, particularly if it crosses multiple departments and specialties. In order to accomplish change it is essential to have a structured and well-defined process, as set out in the toolkit. It describes the five phases of an improvement journey from defining the problem within your own local context, developing a shared purpose within your unit and team, to planning, implementing and testing and measuring, and finally ensuring change is embedded and sustained.
Phase 1: Define the problem
Where are we now?
It is important to understand your local data, and benchmark where possible in the context of regional and national standards. Supporting MBM provision and later breastfeeding, is a complex multidisciplinary intervention. Understanding barriers and shaping effective solutions requires input from all team members across maternity and neonatal care – everyone’s view is valid and essential. Exploring parental perspective and feedback can be very insightful (FIGURE 4).
FIGURE 4 Exploring parental perspective can help with understanding barriers and shaping effective solutions.
It can be useful to brainstorm barriers to each of the five core elements and explore enablers that could work in your unit (TABLE 2). It can also be helpful to speak to other units about how they have identified barriers and enablers and subsequently implemen-ted QI projects to optimise early MBM for preterm babies. High performing units and those who have made significant improvements over time can be identified from NNAP online.
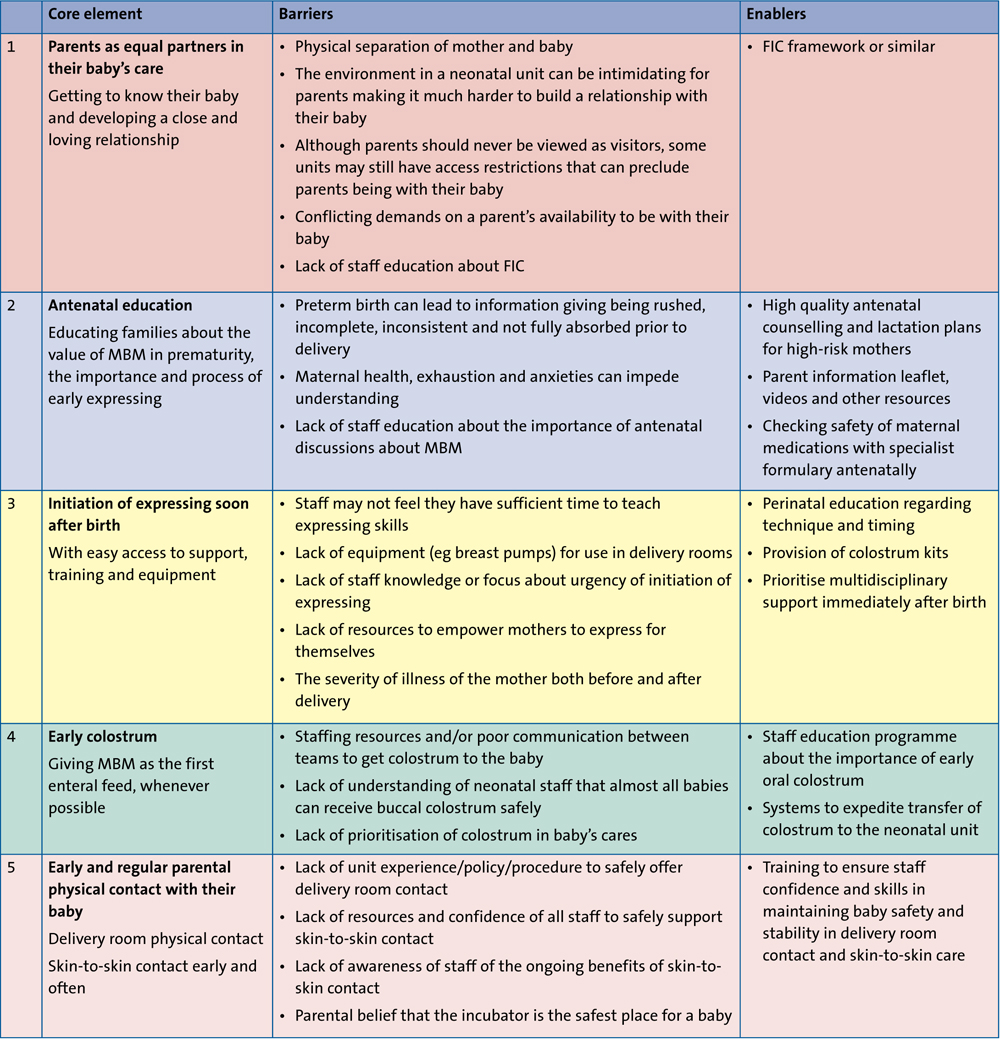
TABLE 2 Barriers and enablers.
Phase 2: Develop a shared purpose
One of the key components to any successful project is having an implementation team that are engaged, resilient, enthusiastic and committed to working together to create the right culture for change.17 Developing a strong multidisciplinary QI team within your workplace will help facilitate communication, understanding and collaboration across departments and allow more cohesive implementation and embedding of the core interventions. Having shared goals, a shared vision and sharing experience ensures your project has momentum and that barriers and enablers can be best appreciated and tackled. It is vital to include the parental voice as their views give a different perspective and their stories form powerful tools for engagement and action.
Phase 3: Plan and implement changes
Consider constructing a ‘project charter’ at the start of this phase to detail your proposed improvement, including the resources required and the potential benefits to patients. A project charter is a format endorsed by many trust improvement teams; it will provide direction and a sense of purpose and may give your project increased leverage with management.
There are a number of methodologies that can be adopted to implement a QI strategy. What matters most is having a consistent approach that you are familiar with and skilled in applying. The Model for Improvement (plan, do, study, act – PDSA) is a widely recognised approach within health care and is frequently associated with positive outcomes for improvement. The toolkit describes how this approach can be used to help implement change ideas for optimising MBM and signposts the BAPM online resources to support this process.
Phase 4: Test and measure improvement
Improvements need to be tested, reviewed and re-tested through a series of PDSA cycles to decide what works and what does not. Improvement is a continuous process that necessitates regular measurement. The toolkit provides examples of outcome, process and balancing measures as they relate to optimisation of early MBM. Sharing data across the whole perinatal team can be very useful, especially if displayed in an accessible, concise and impactful format (FIGURE 5).
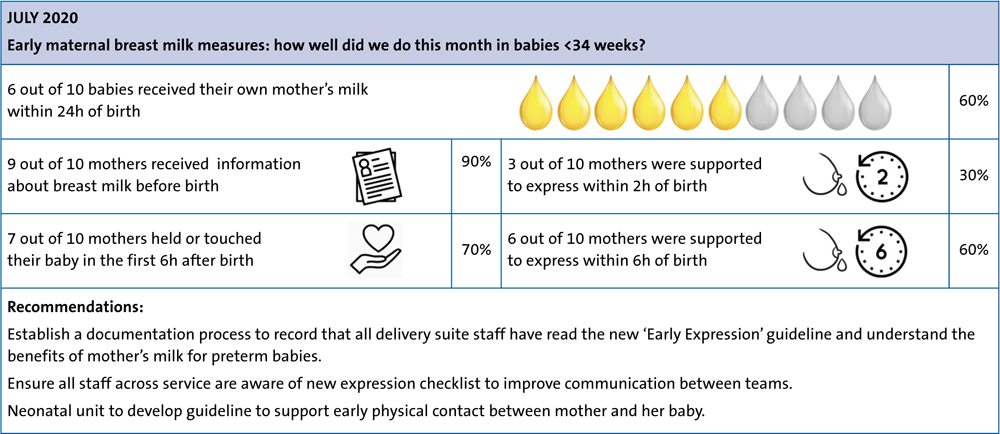
FIGURE 5 Example of staff feedback poster for MBM.
Phase 5: Implement, embed and sustain
This is where change becomes embedded in routine practice throughout the system and is sustained. It is important to implement robust governance arrangements with an early recognition of barriers and loss of motivation. Education is a key element of overcoming barriers particularly within an interactive forum. Use opinion leaders to influence others within your staffing structure and reminder systems to prompt clinicians and the MDT. Ensure feedback of data to staff in a format that they find useful, using impactful stories from families and learning from high achieving units. These methods can help to reinvigorate and embed your changes for improvement.
Summary
Initiating, maintaining and supporting longevity of MBM provision for preterm babies is vital with substantial long-term benefits. Those working in neonatology should be encouraged to foster a collaborative perinatal environment, working hand in hand with parents so that more preterm babies are fed an exclusive human milk diet on their neonatal journey. The holistic, multidisciplinary and family-centred approach to this cannot be over emphasised. The MBM toolkit for preterm infants and its associated resources will support units to develop and implement specific and pertinent QI projects to improve access to MBM for those preterm infants whose outcomes we aim to improve.
Acknowledgements
This toolkit was developed by an MDT representing all areas of the perinatal pathway including midwives, neonatal nurses, neonatologists, infant feeding specialists, speech therapists, dietitians and parent representatives: Sarah Bates, Great Western Hospitals NHS Foundation Trust and BAPM Executive Committee; Julie-Clare Becher, Royal Infirmary of Edinburgh and BAPM Quality Collaborative Lead; Gillian Bowker, NHS Greater Glasgow and Clyde; Cathy Budd, North Bristol NHS Trust; Sara Clarke, West Midlands Neonatal ODN; Lindsay Cracknell, Parent Representative; Aniko Deierl, Imperial College NHS Healthcare Trust; Kate Dinwiddy, BAPM Chief Executive; Cora Doherty, University Hospital of Wales; Kelly Harvey, North West Neonatal ODN; Marcus Hook, BAPM; Genevieve Howell, Parent Representative; Minesh Khashu, Poole Hospital NHS Foundation Trust; Ilana Levene, University of Oxford; Jo Marks, Professional Lead for Speech and Language Therapy; Tanya Miles, Great Western Hospitals NHS Foundation Trust; Nicola Williamson, Parent Representative. Parent Representatives were recruited with generous assistance from Bliss.
To find out more about the BAPM Maternal Breast Milk Toolkit visit: www.bapm.org/pages/196-maternal-breast-milk-toolkit
Or read this article in our
Tablet/iPad edition
