

Neuroprotection: a guide to the latest equipment
In this issue of Infant, we examine the latest medical equipment for supporting neuroprotection in newborn babies. Hypoxic-ischaemic encephalopathy (HIE) is a condition of altered neurological state resulting from a critical lack of blood flow and oxygen to the brain around the time of birth. HIE is a major cause of death and life-long disability and preterm infants are especially at risk for intracranial ischaemic and haemorrhagic injuries. One of the major advances in neonatal care in recent years has been the introduction of therapeutic hypothermia to treat infants with HIE but there are still a number of challenges to managing these infants, particularly with regard to early identification of those infants who may benefit from cooling, monitoring cerebral activity and identifying seizures. Electroencephalography (EEG) remains one of the most useful tools for the diagnosis and prognosis of perinatal cerebral injury. The recent emergence of cerebral oximetry has provided a practical method to measure alterations in cerebral blood flow, which may enable the early detection and prevention of permanent neurological damage.
CerebraLogik simultaneously records EEG and aEEG
The CerebraLogik is a dual-channel differential EEG amplifier that has a clip for attachment to a basinet or patient bed. The CerebraLogik interfaces with the VitaLogik monitor via a cable and can be activated using the universal interface module menu. The display shows real-time EEG with a panel of three hours of amplitude-integrated EEG (aEEG). The aEEG is a filtered and compressed EEG trend that can be used for long-term monitoring of brain function in patients and is increasingly used in high-risk newborn infants. The main indications for aEEG monitoring include early evaluation of brain function after perinatal asphyxia and seizure detection.
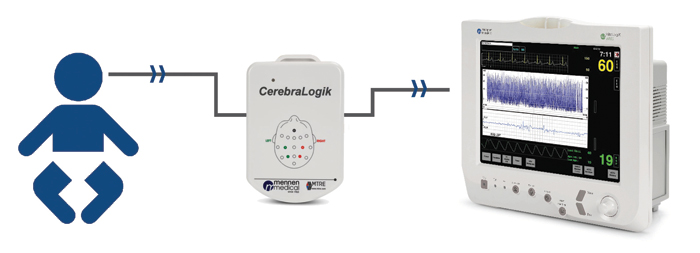
Both EEG and aEEG can be monitored and stored simultaneously with other vital signs scrutinised by the VitaLogik monitor. EEG and aEEG data can be exported from the monitor to a USB stick during and after a procedure (via the USB connector on the monitor) and transferred to a computer. The CerebraLogik viewer software displays the data and, in this way, allows remote viewing of aEEG sections or the complete procedure. CerebraLogik and VitaLogik are available from Charter-Kontron Ltd.
nëo aEEG: optimised monitoring for the NICU
The nëo aEEG monitor from Central Medical Supplies is designed for simple integration into the neonatal unit. With a streamlined set-up to initiate monitoring or review sessions, it is intended for aEEG and EEG monitoring of pathological term and preterm babies.
With up to eight channels, nëo can record rich data in the background, while two aEEG channels are shown for routine monitoring. This allows clinicians to review valuable information whenever needed, without waiting for additional recordings during the critical phases.
Interpreting the numbers with INVOS cerebral/somatic oximetry system
The INVOS system is designed to provide actionable trending values to support clinical decisions on when to intervene. These first alerts rely on speed of reaction and magnitude of response under clinically relevant scenarios.
In neonates, infants and children, cerebral and somatic regional oxygen saturation (rSO2) values provide non-invasive indications of oxygen changes in the cerebral and peripheral circulatory systems. These values may give an early indication of oxygen deficits associated with impending shock states and harmful effects.

The rSO2 value is expressed as a real-time numerical value and a percent change from baseline. With the patient serving as his/her own control – either can be used to customise patient assessment, decision-making and interventions. The balance of perfusion distribution in premature neonates depends on gestational age, day of life and comorbidities. Simultaneous cerebral/somatic rSO2 monitoring can help balance cardiac performance and peripheral perfusion to avoid no- and low-flow states associated with shock and other complications.
Typical cerebral – high blood flow, high O2 extraction:
- typical rSO2 range = 60 to 80, assuming SpO2 is >90
- common intervention trigger is rSO2 <50 or 20% change from rSO2 baseline
- critical threshold is rSO2 <45 or 25% change from rSO2 baseline.
Typical somatic – variable flow, lower O2 extraction:
- variances in the cerebral-somatic relationship may indicate pathology
- watch for drops of 20% below patient baseline.
Available from Medtronic, INVOS technology is designed to meet clinical demands and is backed up by peer-reviewed clinical research.
The therapeutic window for induced hypothermia is within grasp using CritiCool
In their 2019 article, Neonatal Encephalopathy and Hypoxic-ischaemic Encephalopathy, Gunn and Thoresen discuss compelling evidence that mild to moderate induced hypothermia improves survival and neurodevelopmental outcomes. They also review the highly consistent evidence that hypothermia must be started as early as possible.1

Being prepared to quickly manage and initiate treatment can be a challenge. Neonatal staff gain great advantage if the temperature regulation device is easy to operate and trusted. With minimal buttons to press and an intuitive touchscreen that clearly displays all that is needed, CritiCool makes it extremely quick and easy to get started. Integrated with the CritiCool is the CureWrap garment, which wraps around the patient. CureWrap’s versatility and flexibility permits full access to the baby, facilitates repositioning and allows parents to hold their newborn without interrupting cooling.
CritiCool was used to cool infants safely within three hours of birth in a landmark study from 2013 that determined cooling should be initiated as soon as possible after birth in eligible infants.2
Widely used in more than 50 countries, CritiCool is trusted to help neonatal teams around the world effectively control and manage therapeutic hypothermia. CritiCool and CureWrap are available from Belmont Medical Technologies.
References
- Gunn and Thoresen. Neonatal encephalopathy and hypoxic–ischemic encephalopathy. Handbook of Clinical Neurology. 2019 vol 162, chapter 10; Neonatal Neurology.
- Thoresen M, et al. Time is brain: starting therapeutic hypothermia within three hours after birth improves motor outcome in asphyxiated newborns. Neonatology 2013;104:228-33.
Enhancing neurological monitoring of critically ill infants using Unique+
The Unique+ cerebral function monitor (CFM) from Inspiration Healthcare enables simple connectivity of electrodes with LED guides for single or dual-channel use. The user interface offers full touchscreen operation. Optional video can be synchronised to record physical movement as well as electrical activity in the brain. The Unique+ CFM can generate patient reports that can be stored in the hospital network and reviewed remotely.

Or read this article in our
Tablet/iPad edition
