

Quiz: A newborn with arrhythmia – thinking beyond conduction pathways
Consultant Neonatologist
Princess Royal Hospital, The Shrewsbury and Telford Hospital NHS Trust
sagarika.ray@nhs.net
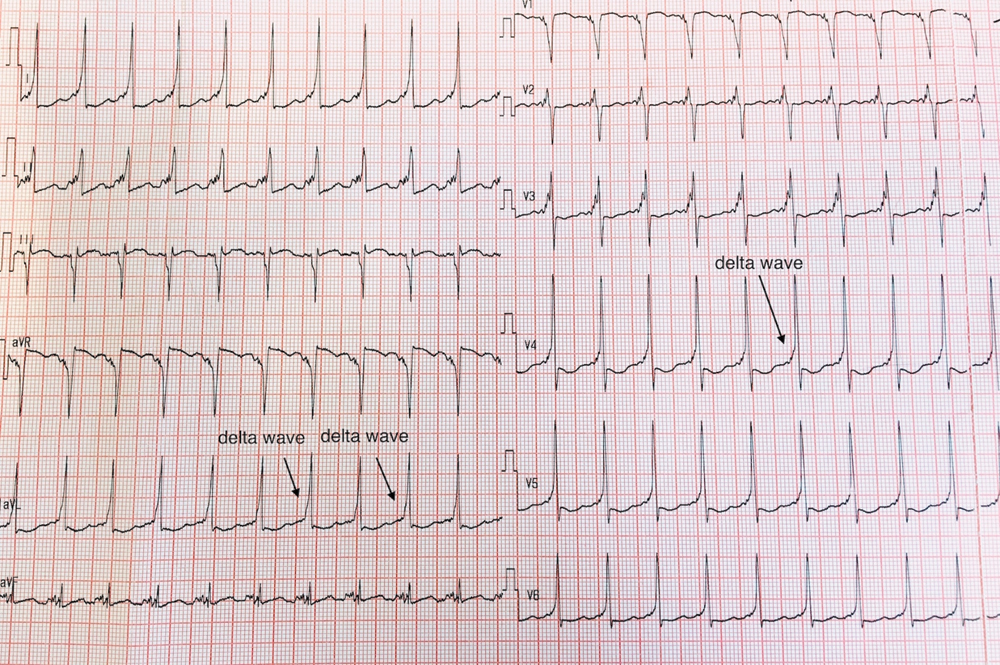
FIGURE 1 shows the baseline 12-lead electrocardiogram (ECG) of a term baby after management was initiated for a narrow-complex tachycardia with a heart rate >250bpm. An echocardiogram revealed multiple cardiac rhabdomyomas affecting the atria, ventricles and anterior leaflet of the tricuspid valve, causing intermittent obstruction.
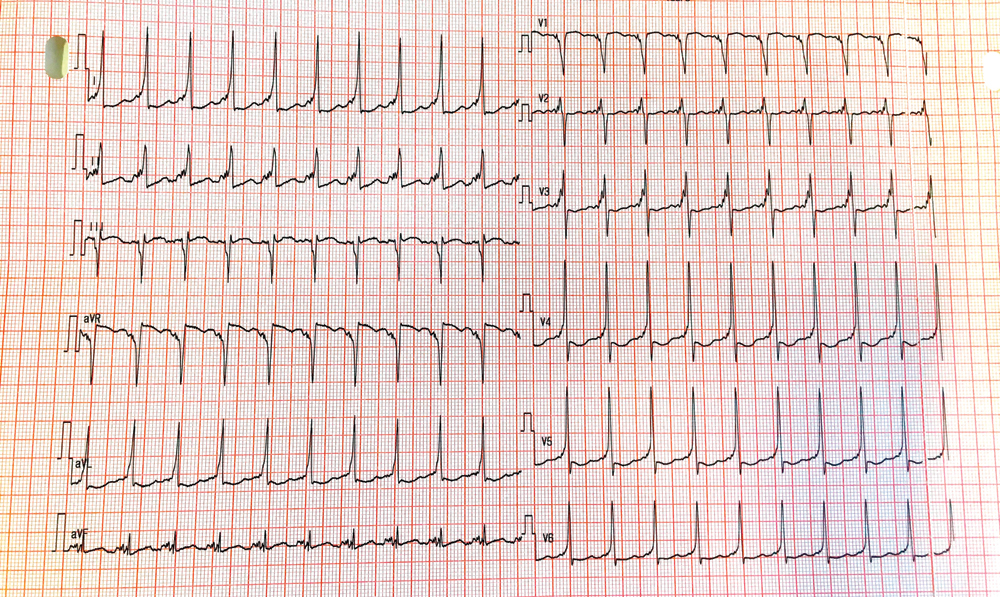
FIGURE 1
1. What condition is shown in FIGURE 1
- Junctional ectopic tachycardia
- Atrial flutter
- Wolff-Parkinson-White (WPW) syndrome
- Complete heart block
- Atrial fibrillation
2. Which of the following is not included in the immediate management of the narrow complex tachycardia?
- 24-hour ECG recording
- Umbilical venous catheterisation
- Synchronised DC cardioversion
- Ice pack on face
- Adenosine
3. What condition can cardiac rhabdomyomas and the underlying arrhythmia be associated with?
- Neurofibromatosis
- Tuberous sclerosis complex
- Von Hippel-Landau disease
- Li-Fraumeni syndrome
Answers
1. The correct answer is (c)
The ECG shows features of Wolff-Parkinson-White (WPW) syndrome as there is pre-excitation with a short PR interval and a delta wave (slurring of the upstroke of the QRS complex), as noted in FIGURE 1.
2. The correct answer is (a)
The management of narrow complex or supraventricular tachycardia (SVT) includes initial assessment of the infant for cardiovascular stability and the presence of shock, along with measures for terminating the episode.1 If unstable or shocked, they will need synchronized DC cardioversion. Stable infants will need the termination of the SVT through vagal manoeuvres (ice pack on the face) or pharmacological measures. Intravenous access in a large vein as close as possible to the heart should be attempted. In the newborn, the umbilical vein provides easy access to the inferior vena cava. Intravenous adenosine is the pharmacological mainstay and needs to be followed by a quick flush in view of its very short half-life (<10 sec) and its inactivation by adenosine deaminase in the bloodstream. Subsequent 24-hour ECG recording may be helpful for detection of further episodes and to aid in diagnosis.
3. The correct answer is (b)
Tuberous sclerosis complex (TSC) is a genetic syndrome that presents with cardiac rhabdomyomas and has associations with WPW syndrome.2 The other conditions mentioned include hereditary cancer syndromes and neurocutaneous syndromes, which do not typically present with these features. About 70-90% of children with rhabdomyomas have TSC. Cardiac rhabdomyomas are often multiple and can cause haemodynamic effects, congestive cardiac failure, and outflow obstruction. They tend to regress spontaneously, although surgical resection may be needed in some cases of haemodynamic compromise. Cardiac arrhythmias are a significant and relatively common problem in TSC and can vary from slow to irregular to fast heart rhythms. They may result from cardiac rhabdomyomas or in isolation. Hence, it is recommended to obtain a baseline ECG in individuals of all ages with TSC and at regular intervals to assess for underlying conduction defects.3,4
Or read this article in our
Tablet/iPad edition
