

Arachnoid cyst: a review and report of two rare cases
Arachnoid cysts are benign fluid-filled sacs that develop on the arachnoid membrane in the brain or spinal cord. Most arachnoid cysts are stable and do not cause any symptoms throughout an individual’s life; others can put pressure on the brain because of a mass effect. With advances in imaging modalities, it is now possible to identify arachnoid cysts in antenatal scans. This article reviews arachnoid cysts in the neonatal period via two case reports.
Barbara PaqueteMD, MRCPCH
ST4 Paediatrics
barbara.paquete@nhs.net
Katie McArthur
MBChB, MRCPCH
ST7 Paediatrics
Sanjeev Rath
MBBS, MD, FRCPCH
Consultant Neonatologist
Anna Paweletz
MD, MRCPCH
Consultant Neonatologist
Arrowe Park Hospital, Wirral University Teaching Hospital NHS Foundation Trust
Case reports
We report two cases of arachnoid cysts recently encountered in the neonatal intensive care unit at Arrowe Park Hospital. Both cases were antenatally diagnosed, confirmed postnatally and are being managed conservatively with input from the paediatric neurosurgical team.
Case 1: a 30-year-old multiparous woman
An anomaly ultrasound scan (USS) at 20 weeks of pregnancy was normal; a repeat scan performed at 34+3 weeks to monitor growth showed an intracranial cyst measuring 14x13mm. The mother was referred to the fetal medicine unit (FMU) where a USS at 36+4 weeks showed an intracranial cystic lesion that measured 17x20mm in size and was diagnosed as an arachnoid cyst. A further scan at 37+2 weeks confirmed the findings.
The woman delivered a healthy baby weighing 3.14kg at 37+5 weeks’ gestation. On day 2, a postnatal USS showed a large cystic lesion measuring 17x17mm, adjacent to the midbrain along with a small cystic lesion adjacent to the caudothalamic notch. A review of scans and discussion with the local tertiary paediatric neuro-surgical centre supported the diagnosis of suprasellar arachnoid cyst. As the baby was clinically stable, the neonatal team was advised to monitor the head circumference weekly, arrange an outpatient magnetic resonance imaging (MRI) of the brain and perform blood tests for karyotyping and DNA microarray analysis.
The outpatient MRI performed on day 6 of life FIGURE 1 showed a large suprasellar arachnoid cyst 18x22mm in size, which was causing a significant mass effect in displacing and compressing the midbrain (more marked on the left side) and basal ganglia. The third ventricle was distorted; the pituitary stalk and optic nerve were stretched across the anterior and right superolateral surface of the cyst; septations were seen within the right side of the cyst with no cerebrospinal fluid (CSF) flow identified across the cerebral aqueduct on a CSF flow study. The ventricles were not dilated. The cerebral cortex, cerebellum, cerebellar vermis and the corpus callosum appeared normal. No abnormal MRI signal was identified within the brain parenchyma and myelination was reported as age appropriate.
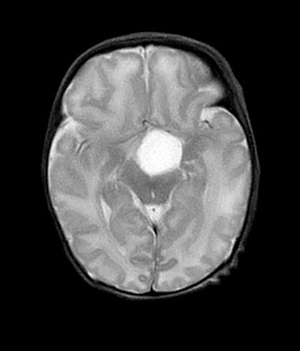
FIGURE 1 Case 1: a large suprasellar arachnoid cyst.
Following the MRI review, the neurosurgical team advised no urgent treatment. An ophthalmology appointment was arranged as were weekly head circumference measurements and urea and electrolyte biochemistry tests (for monitoring of sodium). Open access was arranged to the paediatric ward and the parents were educated about warning signs and when to seek urgent medical attention. A second MRI at four weeks of age showed similar findings to previously. A TORCH screen (note, TORCH originally stood for toxoplasma, rubella, cytomegalovirus and herpes, however, the acronym is outdated and herpes serology is no longer performed) and microarray analysis were normal, and the ophthalmological physical examination did not find any abnormality.
At the neurosurgical clinic at five weeks of age, the child’s head circumference was between the ninth and 25th centile. There were no clinical signs of raised intracranial pressure. As the second MRI did not show hydrocephalus, the agreed plan was for conservative management with input from the endocrine team. The endocrine team assessed dynamic hormone tests for pituitary dysfunction (adrenocortico-trophin hormone, short synacthen (corticotropin) test, thyroid function tests, renal profile tests, random blood sugar tests and insulin-like growth factor-1) and these were all normal.
At the nine-month follow-up appointment with the neurosurgical team, the infant was developing normally. The head circumference showed an increase from the 50th to the 98th centile and so a third MRI was performed; this showed no significant changes. To date, the infant remains well with no features of raised intracranial pressure and no hydrocephalus. The plan is to conduct close follow-up at three to four month intervals.
Case 2: a 34-year-old multiparous woman
The anomaly USS at 20 weeks of pregnancy was normal. A growth scan at 28+1 weeks showed asymmetric ventriculo-megaly with an enlarged right ventricle measuring 24mm, which led to referral to the FMU. A repeat scan at 28+2 weeks showed a left sided 25x33mm intracranial cyst (likely arachnoid in nature).
A follow-up scan at 32+1 weeks of pregnancy showed similar findings. The woman underwent a joint FMU/neurosurgical counselling session with a plan that following birth the baby would be seen as an outpatient at the regional tertiary neurosurgical centre within the first few weeks of life and would have weekly head circumference measurements by the local neonatal community team. An antenatal scan at 37+1 weeks revealed that the condition of the cyst had remained unchanged.
A postnatal cranial ultrasound performed on day 3 of life showed a large arachnoid cyst 37x47mm in size on the left posterior area of the brain. The baby was followed as per the advice from the neurosurgical team. At the neurosurgical clinic, MRI showed the cyst to be stable in size; the infant’s head circumference measured between the 91st and 98th centiles (previously 75th). The infant was developing normally.
The most recent MRI at the age of one year FIGURE 2 showed the presence of the cystic lesion in the left occipitoparietal region measuring 60x60x71mm (previously 42x48x58mm). The CSF signal intensity was followed on all sequences with no restricted diffusion or susceptibility noted. A thin septum was seen along its posterior wall and a further tiny cyst beyond the septation. This remained unchanged from previously. This caused mass effect and distortion of the corpus callosum (body and splenium), the third and left lateral ventricles; the left occipital and temporal horns showed moderate dilatation and the third ventricle was mildly dilated. Mild mass effect was also noted on the posterior aspect of the left thalamus, lateral aspect of the left cerebral peduncle and the superior aspect of the left cerebellar hemisphere. There was also displacement of the internal cerebral veins and the vein of Galen, although a signal void was preserved implying flow within the vessels. This was similar to the previous scan. There was no restricted diffusion to suggest acute infarct or susceptibility to intracranial haemorrhage. The midline structures appeared normal, including the corpus callosum (allowing for displacement), pituitary, optic chiasm and craniocervical junction. The foramen magnum was patent.
The baby remains under close follow-up with monitoring by the neurosurgical team.
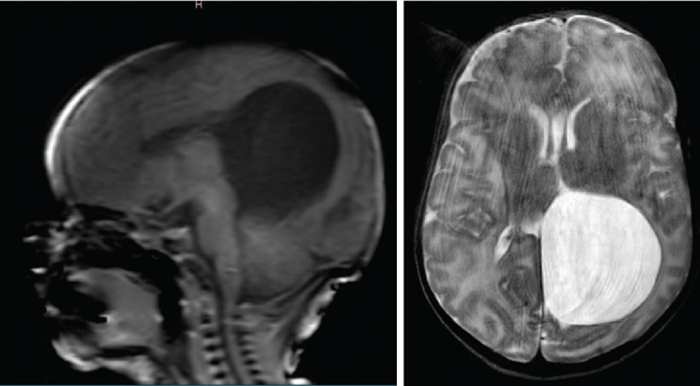
FIGURE 2 Case 2: the large occipito-parietal arachnoid cyst showing the intracranial mass effect.
Review and discussion
Arachnoid cysts are benign cysts that occur in the cerebrospinal axis in association with the arachnoid membrane. They are most commonly developmental anomalies; however, some are acquired. Congenital (or primary) arachnoid cysts are filled with fluid similar to CSF and formed due to congenital splitting of the arachnoid layer. Secondary arachnoid cysts are rare and can form following infection, haemorrhage, trauma or surgery.1 Arachnoid cysts represent 1% of all space-occupying lesions in childhood. The cysts are commonly
(50-60%)2 identified incidentally in the supratentorial region (middle cranial fossa or Sylvian fissure), as in the second case presented here.
The suprasellar location, seen in our first case, is less common, accounting for 10% of all arachnoid cysts. Cysts in the middle cranial fossa are found more frequently in boys than in girls and they are more frequent on the left side. Enlargement of the cyst can lead to hydrocephalus, visual impairment or endocrine dysfunction.3
With the development of better antenatal diagnostic tools (eg ultrasonography and fetal MRI), most arachnoid cysts are now diagnosed before birth in the second trimester, or even as early as 20 weeks of pregnancy. In our cases, the diagnoses were made a little later on growth scans. If not detected antenatally, arachnoid cysts are often diagnosed in childhood when symptoms appear.4
Arachnoid cysts in the antenatal period can be found in isolation with no other intracranial abnormalities. However, cysts located in the suprasellar region can be associated with other intracranial findings, such as hydrocephalus, agenesis of the corpus callosum and, less commonly, hypothalamic hamartomas.5 Obstructive hydrocephalus occurs in up to 90% of patients with suprasellar arachnoid cyst, despite this we are yet to see hydrocephalus and associated features in our first case.
An antenatal diagnosis should be confirmed by neonatal neuroimaging; cranial ultrasonography is the first line imaging modality and should happen within the first 24 hours of birth. The findings should then be confirmed by a more thorough brain MRI that ideally should be carried out within the first couple of weeks of life.6 Antenatally diagnosed arachnoid cysts may remain clinically silent in the postnatal period or even regress spontaneously. They have a tendency to grow rapidly in size during the second or third trimester and in the postnatal period, when they can occasionally become symptomatic. This has not happened within the first year of life in either of our cases.
There is no clear guidance on the most appropriate management strategy of antenatally diagnosed arachnoid cysts. Some clinicians recommend treating only those cysts that cause symptoms; others recommend treating asymptomatic cysts to avoid future complications.7 Management approaches include:
- endoscopic/microscopic fenestration of the cyst
- cystoperitoneal shunt
- cystocisternostomy
- cystoventriculostomy
- ventriculocystocisternostomy.
Endoscopic ventriculocystocisternostomy seems to be the preferred approach.8
Outcomes are variable. An isolated small cyst is unlikely to have any impact on neurodevelopment, whereas a large and compressing cyst requires surgery to prevent longterm sequelae.9 The outcomes are improved with a normal karyotype and in the absence of other developmental anomalies, which so far appears to be the case for both of our babies.
Conclusion
Arachnoid cysts are rare and can remain asymptomatic during childhood. With advancement in imaging modalities, it is now possible to identify these cysts antenatally. Rapid enlargement of incidentally diagnosed antenatal arachnoid cysts can occur in the perinatal period. Serial evaluation by imaging in the perinatal period is necessary to demonstrate any rapid cyst enlargement and the need for appropriate intervention/management. The neurosurgical approach regarding antenatally diagnosed arachnoid cysts is variable, however, cysts that occur in isolation without any other intracranial anomalies and a normal karyotype usually have a good outcome.
Parental consent
The authors received written consent from the parents to publish these case reports.
Or read this article in our
Tablet/iPad edition
- Rapid enlargement of antenatally diagnosed arachnoid cysts can occur in the perinatal period.
- Appropriate postnatal management usually leads to a good outcome (in the absence of other intracranial anomalies and a normal karyotype).
- Treatment, if necessary, involves draining the fluid through surgery or shunting.
