

Cardiorespiratory events after first vaccination of preterm infants born before 33 weeks’ gestation
This comparison study was designed to determine if preterm infants (<33 weeks’ gestation and already discharged from hospital), are at risk of developing cardiorespiratory events (CREs) after their first routine vaccination at the chronological age of two months. Participants received a 10-valent pneumococcal conjugate vaccine and a combination vaccine for diphtheria, acellular pertussis, tetanus, polio, Haemophilus influenza B and hepatitis B. The occurrence of clinically relevant CREs was not increased after vaccination. We conclude that preterm infants who have already been discharged from hospital can safely be vaccinated in an outpatient setting at the recommended chronological age of two months without additional cardiorespiratory monitoring.
Daniel Molanus1MD
danielmolanus@gmail.com
Jaap Schilperoort2
MD
Bart Boersma3
MD, PhD
1Department of Paediatrics, Ziekenhuis Amstelland, Amstelveen, The Netherlands 2Department of Paediatrics, Onze Lieve Vrouwe Gasthuis, Amsterdam, The Netherlands 3Department of Paediatrics, Noordwest Ziekenhuisgroep, Alkmaar, The Netherlands
The Dutch National Immunisation Programme, in keeping with inter-national guidelines, recommends vaccination of preterm infants at the appropriate chronological age without correcting for gestational age.1-4 In the Netherlands infants receive their first vaccination, a 10-valent pneumococcal (Pneu) conjugate vaccine and a combination vaccine for diphtheria (D), acellular pertussis (aP), tetanus (T), polio (P), Haemophilus influenza B (HiB) and Hepatitis B (HBV) at six to nine weeks of age. Studies evaluating immunogenicity of these vaccines in preterm infants demonstrate that protective immune responses are often achieved.5-7
It is known that extremely preterm infants born before 28 weeks of gestation are at increased risk of CREs, such as apnoea, bradycardia and/or desaturation, after vaccination.8-21 Risk factors to develop CREs after vaccination include low gestational age and/or low birth weight, a medical history of apnoea of prematurity, intubation, bronchopulmonary dysplasia, other chronic diseases, vaccination at a young age and/or a low weight at the time of vaccination.8-11,13,14,17,18,20 These risk factors were identified in studies where infants were still inpatients in the neonatal ward, with cardiorespiratory monitoring at the time of their first vaccination.
However, for moderately preterm infants that have already been discharged from the hospital by the time of their first vaccination, it is less clear whether there is an increased risk to develop CREs after routine vaccination. Uncertainty exists whether these infants can safely be vaccinated in an outpatient setting without the need for close monitoring or readmission to the hospital. This pre-/post- intervention comparison study investigates if CREs occur after the first routine vaccination of preterm infants born before 33 weeks of gestational age who have already been discharged from hospital.
Materials and methods
This pre-/post-intervention comparison study was conducted from July 2013 to January 2018 with the approval of the Medical Research Ethical Committee Noord-Holland, Alkmaar, the Netherlands (Clinical trial registry name and registration number: Cardiorespiratory disturbances after 1st vaccination in premature infants. METC registration number: M012-029. CCMO registration number: NL35641.094.12).
Preterm infants born before 33 weeks’ gestation who had already been discharged from the High Care Neonatology Department of the Northwest Hospital Group in Alkmaar, the Netherlands, at the time of their first routine vaccination were eligible to participate. Exclusion criteria were: hospital admission at the time of the first vaccination for reasons other than participation in this study; need for respiratory support or tube feeding at home; any known congenital or acquired medical condition affecting cardiorespiratory stability at the time of vaccination, and lack of written parental consent.
Participants were readmitted at the chronological age of approximately two months and monitored continuously for heart rate, respiratory rate and transcutaneous oxygen saturations using a Philips IntelliVue MP70 monitor. After an 18-hour pre-intervention monitoring period all participants received their first vaccination at 9am, which consisted of a Pneu conjugate vaccine, Synflorix, (GlaxoSmithKline Biologicals, Belgium) and a combination vaccine, Infanrix hexa, (GlaxoSmithKline Biologicals, Belgium) for D-T-aP-HBV-P-HiB in accordance with the Dutch National Immunisation Programme. Post-vaccination monitoring continued for 24 hours.
Disturbances in cardiorespiratory parameters were described in detail by the nursing staff using a standardised form and a registration of the event was printed from the monitor. Afterwards these events were assessed by all authors independently to determine if the disturbance met the criteria for a CRE, including apnoea, bradycardia or desaturation. The authors were blinded to participant identity and clinical background, and whether the event occurred pre- or post-intervention. There were only minor discrepancies in interpretation of events between the assessors and these were resolved after discussion.
An apnoea was defined as an isolated respiratory arrest of ≥20 seconds or a respiratory arrest ≥15 seconds combined with a heart rate <80 beats per minute for ≥5 seconds.22 A bradycardia was defined as a heart rate <80 beats per min for ≥20 seconds. Desaturation was defined as a transcutaneous measured oxygen saturation <86% during ≥15 seconds.
A CRE was defined as ‘mild’ if the event resolved spontaneously without the need for intervention. A CRE was defined as ‘significant’ if the event did not resolve spontaneously and required intervention such as tactile stimulation, oxygen supple-mentation or other respiratory support.
Primary outcome was the within-subject comparison of the occurrence of CREs before and after vaccination. Secondary outcome measures were the pre- and post-intervention comparison of the occurrence of other adverse reactions such as fever, local skin reactions, gastrointestinal symptoms and discomfort.
Statistical analysis was performed using IBM SPSS Statistics Version 25. Descriptive statistics were used to describe the parti-cipant characteristics. Primary and secon-dary outcome analyses were performed using McNemar’s test and the Wilcoxon signed-rank test. Correction was made for the difference in observation duration pre- and post-intervention. P <0.05 was considered statistically significant.
Results
The flowchart in FIGURE 1 shows the study design and participant enrolment. In total, 88 patients were eligible for participation, of which 52 were enrolled. In 35 cases informed consent was refused, mostly because of the need for admission for two consecutive nights. One infant was excluded because of prior admission for a brief unexplained event at home.
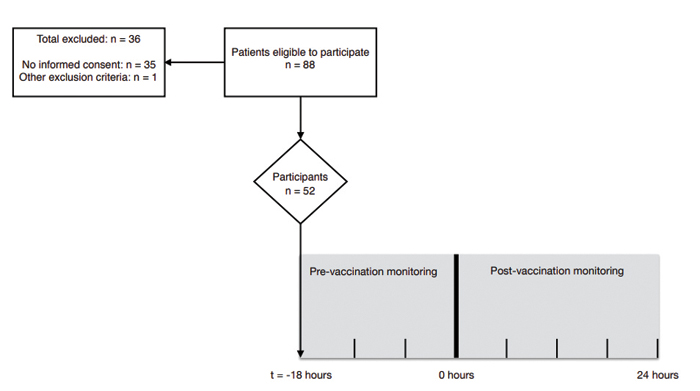
FIGURE 1 Study design and flowchart of participant enrolment. At 0 hours the participants received a 10-valent Pneu conjugate vaccine and combination vaccine for D-T-aP-HBV-P-HiB.
Participants’ characteristics are shown in TABLE 1. The mean gestational age was 31 weeks and 3 days. The mean birth weight was 1,660g (range = 990-2,580g). The medical history of participants included intubation (13%), pharmacological treatment for apnoea of prematurity (65.5%), intraventricular haemorrhage (11.5%) and neonatal sepsis (5.7%).
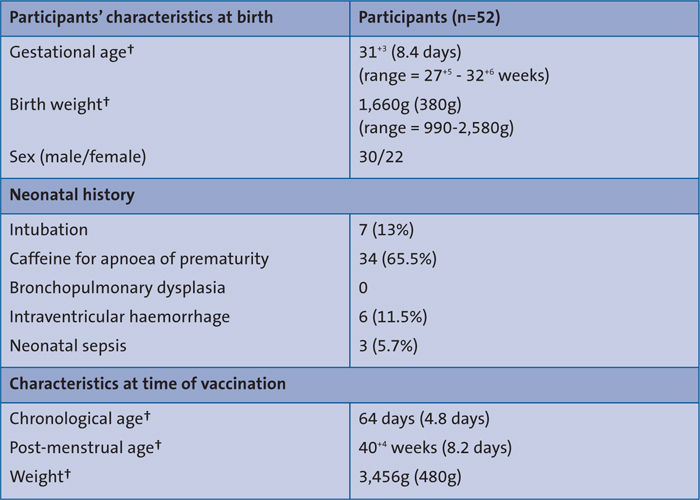
TABLE 1 Participants’ characteristics. †mean (error measures).
None of the participants fulfilled the criteria for bronchopulmonary disease. At the time of the first vaccination the mean chronological age was 64 days (range = 50-75 days), the mean post-menstrual age was 40+4 weeks (range = 37+1-43+3 weeks) and the mean weight was 3,456g (range = 2,405-4,910g).
The vast majority, 47 out of 52 infants, developed no CREs during the observation period of this study. Three infants developed CREs after they received their first vaccination; they had none beforehand. Two of these three infants developed one CRE each that resolved spontaneously. One infant, born at a gestational age of 31+5 weeks with a birth weight of 1,800g, experienced one mod-erate CRE associated with an obstructive incident during feeding – as evidenced by desaturation in combination with increased thorax excursions and tachycardia. The infant recovered after feeding was withdrawn and tactile stimulation was given by the nurse.
Two infants showed CREs both pre-and post-vaccination. One of these infants showed multiple moderate CREs requiring tactile stimulation. This infant was born at a gestational age of 28+6 weeks with a birth weight of 1,220g. His neonatal history was unremarkable except for caffeine treatment for apnoea of prematurity. He was also diagnosed with gastro-oesophageal reflux prior to this study. Review of these CREs showed they were all related to feeding. The other infant showed one CRE before vaccination and three CREs after vaccination. These CREs were central apnoea in nature and all resolved spontaneously. This infant, born at a gestational age of 32 weeks with a birth weight of 1,717g, had a history of intubation and had received caffeine treatment for apnoea of prematurity.
Statistical analysis found no significant increase in the number of participants with CREs after vaccination (p-value = 0.250). The total number of CREs was signifi-cantly increased from eight CREs prior to vaccination and 18 CREs post-vaccination (p-value = 0.041). However, the number of ‘significant’ CREs was not significantly increased, with four significant CREs observed before vaccination compared to eight post-vaccination (p-value = 0.180). Notably, the infant previously described with gastro-oesophageal reflux accounted for 69% of all observed CREs (seven CREs pre-vaccination and 11 CREs post-vaccination).
Secondary outcome measurements are shown in TABLE 2. Participants showed a significant increase in temperature above 38.0°C (p-value = 0.001), discomfort (p-value = 0.019) and local skin reaction (p-value = 0.007) after vaccination.
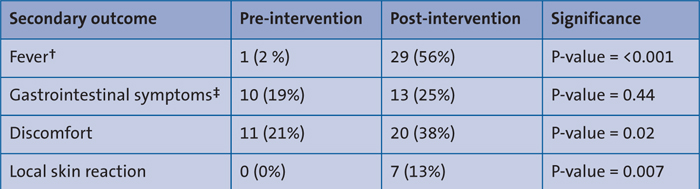
TABLE 2 Analysis of secondary outcome measures pre- and post-intervention using McNemar’s test. †Fever is defined as temperature above 38.0°C. ‡Gastrointestinal symptoms include feeding difficulties, vomiting and/or diarrhoea.
Discussion
In this group of preterm infants born before 33 weeks’ gestation, we found a significant increase in the number of CREs after the first vaccination at the chronological age of approximately two months. However, in all but two infants the CREs resolved spontaneously and were not harmful. The significant, potentially harmful if unnoticed and therefore clinically relevant, CREs in these two infants did not seem to be related to the vaccination since one also experienced significant CREs before vaccination and the other showed one CRE during feeding that was clearly obstructive in nature and would have induced intervention in an outpatient setting as well. Furthermore, the number of significant CREs was not significantly increased after vaccination.
We are aware that the observational study design limits the strengths of our conclusions. However, a randomised controlled design, admitting infants without vaccinating them, was not feasible to perform. Another limitation of our study is the relatively small sample size.
Furthermore, we found that there was no consensus in the literature on the definition of a CRE, apnoea, bradycardia or desaturation, complicating our ability to compare our results with other studies. Most importantly, most studies only included extremely preterm infants that were still admitted to the neonatal ward by the time of their first vaccination, whereas we solely focussed on moderately preterm infants who had already been discharged.8-21 This group understandably has less comorbidity. The only other study, which involved readmitting preterm infants to receive their first vaccination, was also performed at our hospital – with none of the 31 participants suffering significant CREs.10 Furthermore, in keeping with our findings, no association between vaccination and the occurrence of moderate or severe CREs in preterm infants has ever been reported in post-marketing surveillance programmes such as Lareb (The Netherlands Pharmacovigilance Centre) or Vaccine Adverse Events Reporting System (Centers for Disease Control and Prevention, USA). A recent published manufacturer-funded review about safety and immunogenicity of the hexavalent combined D-T-aP-HBV-P-HiB vaccine did report the occurrence of CREs after vaccination in preterm infants.23 However, this review also reported CRE events in term infants and as no control group or sequential data within subjects is available, it is impossible to determine whether these CREs can be attributed to vaccination.
Conclusion
We conclude that for preterm infants born before 33 weeks of gestation who have already been discharged from the hospital, the first routine vaccination at two months of age can safely be administered in an outpatient setting without cardio-respiratory monitoring.
Or read this article in our
Tablet/iPad edition
- Extremely preterm infants are at risk of CREs after their first vaccination and should be monitored in hospital.
- This study shows that preterm infants who have been discharged from hospital are not at increased risk for developing relevant CREs after routine vaccination at two months of age.
