

Managing the difficult neonatal airway: a BAPM framework for practice
This article outlines the British Association of Perinatal Medicine’s (BAPM) framework for practice for managing the difficult neonatal airway. It describes how the framework is intended to be used and implemented to support centres in developing their own approach to the difficult neonatal airway.
Robert TinnionMD, MRCPCH, Consultant Neonatologist
Royal Victoria Infirmary, Newcastle upon Tyne
robert.tinnion@nhs.net
Alan Fenton
MD, MRCP(UK), Consultant Neonatologist
Royal Victoria Infirmary, Newcastle upon Tyne
On behalf of the BAPM Difficult Airway Framework Working Group
Managing the difficult airway in the neonate: a BAPM framework for practice1 was developed by specialists likely to be involved in the management of difficult airways in neonates, using pre-existing guidance (both adult and paediatric) and a literature review, followed by public consultation. The framework makes five key recommendations (TABLE 1).
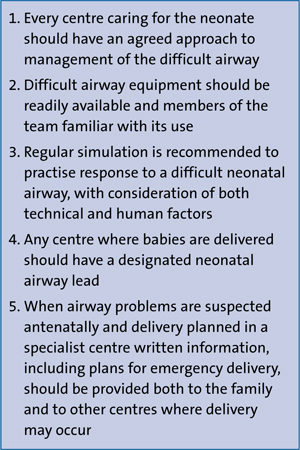
TABLE 1 Framework recommendations for implementation in practice.
The difficult airway
‘To fail to prepare is to prepare to fail’ sums up the management of any difficult airway. In anaesthesia a difficult airway is recognised as an emergency equivalent to resuscitation of an arrested patient. There are international societies such as the Difficult Airways Society (DAS) and a number of widely-taught, standardised approaches dedicated to safely managing the difficult airway. Neonatal medicine has mostly lagged behind in this area: surveys repeatedly show preparation for a difficult airway is patchy at best.2,3 Some specific UK courses do exist for managing the difficult neonatal airway but no single approach is embedded in practice nationally. This BAPM framework provides a resource raising awareness of the difficult airway in neonatal settings and a template for teams to develop an approach appropriate for their circumstances.
The BAPM framework for practice.
Several factors impact on the implementation of a structured, standardised approach to managing the difficult neonatal airway. While the definition of a neonate is until 44 weeks postmenstrual age, there will be older infants in whom a ‘neonatal’ approach is appropriate. Significant variation in expertise and equipment may exist between and within hospitals. Additionally some of the challenges of neonatal intubation, both anatomical and operatordependent,4 may make a straightforward intubation difficult. Thus no single protocol could be mandated nationally applicable to all settings.
The framework implementation process and template algorithm allow any team to assess local resources and formulate their own difficult airway plan, which can be incorporated into local training.
Key principles of framework implementation
Role of the neonatal airway lead
A nominated neonatal airway lead should take responsibility for implementing the framework. The person in the lead role will depend on the location of the particular service. Their responsibilities are set out in (TABLE 2).
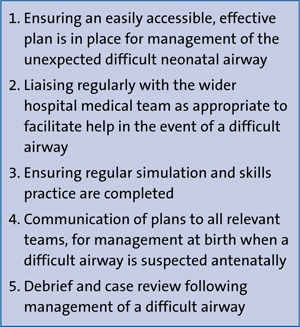
TABLE 2 The responsibilities of the neonatal airway lead.
Implementation of the framework process
For the difficult airway template to work effectively in an emergency situation, three preparatory steps must have occurred that are, primarily, the responsibilities of the neonatal airway lead:
- Assessing available resources
- Compiling equipment and finalising the local framework algorithm
- Training, simulation, and debriefing.
1. Assessing available resources
Expertise in airway management will vary between settings. Likewise colocation of specialist teams will impact on equipment availability. However, all hospitals have resources that can be used to help by thinking ‘outside the box’ in the planning stages. For example, obstetric anaesthetists have transferrable airway management skills. Many anaesthetic departments in the UK have access to a videolaryngoscope (VL). Purchase of neonateappropriate blades to be used with VLs elsewhere in the hospital may remove the need for dedicated neonatal VL equipment. Adult ENT (ear, nose, throat) services may, likewise, be able to help in emergencies.
The framework acknowledges that enlisting non-neonatal specialists raises professional practice issues. Where potential conflict of responsibility, or practice outside the normal scope of practice might occur, advice from relevant professional governing bodies should be taken into account. The designated neonatal airway lead must ensure opportunity is provided for these contributing specialties to have regular neonatalspecific training and simulation.
Equipment options and human factor considerations are given in the resources document accompanying the framework. Wherever possible there should be alignment with equipment used elsewhere in the hospital, allowing continuity and familiarity.
The resources document also provides a description of advanced airway and surgical techniques used by ENT or respiratory specialists in managing the difficult airway. There is no expectation that these techniques will be used by untrained hands, but the information should help inform any discussion across healthcare boundaries about service provision.
2. Compiling equipment and finalising the local framework algorithm
The framework’s template algorithm for local adaptation is available to download free online at: www.bapm.org/resources/199-managing-the-difficult-airway-in-the-neonate.
The front page allows key contact numbers to be listed, and the specific location of key equipment in the depart-ment with instructions on how to retrieve it. Advanced airway and intubation adjuncts should be kept within easy reach of the area in which they are likely to be needed, in a single place to be readily available, but not necessarily used routinely. Other equipment found elsewhere in the hospital can also be listed to minimise delay in obtaining it if needed. There is also a section to list drug doses.
The reverse of this sheet (FIGURE 1) works through plans A-D for the management of the difficult airway. Actions and equipment should be tailored to the equipment and personnel available. This approach emphasises doing the basics well, then structures subsequent intervention to find a point of stability, allowing time to consider definitive intervention. Stability may be found, for example, using mask ventilation successfully (can’t intubate, can ventilate), or by being able to provide some oxygenating respiratory support, accepting ventilation is suboptimal (can’t intubate, can oxygenate). Alternatively the team may be faced with a true ‘can’t intubate, can’t oxygenate’ situation needing addressing with plan C/D. The page is laid out in a similar fashion to that found in the DAS guidance for older patients, maintaining alignment and familiarity for other teams involved.
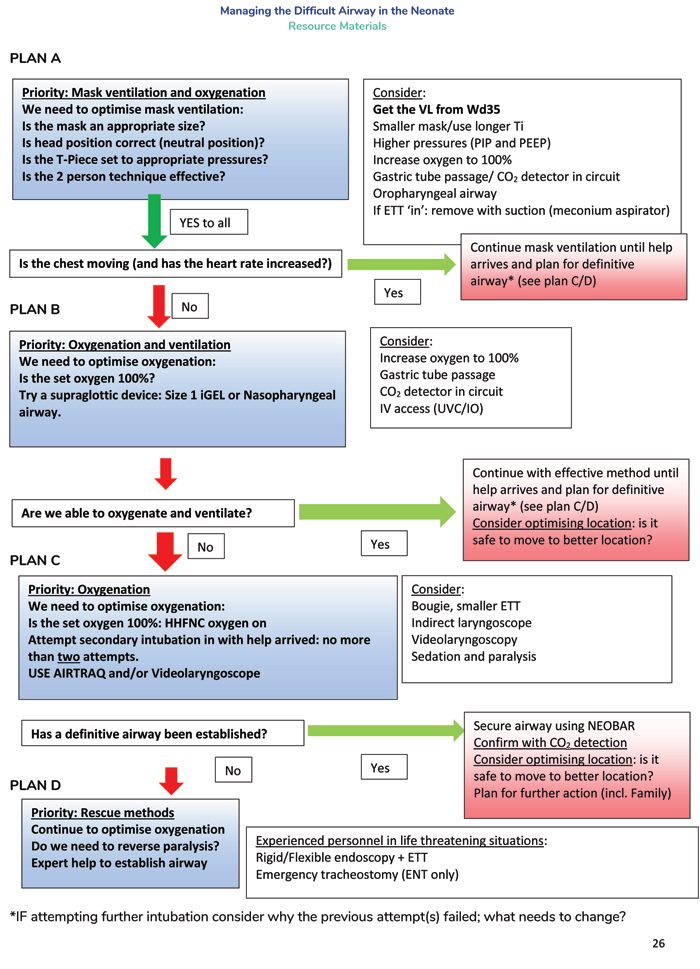
FIGURE 1 Example of a completed algorithm template.
The final page is a separate sheet where labelled photographs of the equipment can be organised in an A-D sequence, allowing prompt identification.
3. Training, simulation, and debriefing
Embedding the process in the organi-sational memory using simulation is key. Once the A-D plan is agreed, a multi-disciplinary simulation session should be coordinated by the neonatal airway lead to test the process and identify any issues. Sessions should be held regularly to maintain skills and responses.
Two key features of simulation are ensuring teams recognise when to ‘declare the emergency’ and then use of ‘challenge and response’ to work through the algorithm. Recognising and declaring a difficult airway situation is essential to ensure the process starts promptly. Delay and task fixation with prolonged intubation attempts cause harm. Once declared, the key algorithm points should be read out loud by a team member (challenge). Those who have ‘hands on’ should respond simply (yes/no) to the questions posed (response), leading the clinical team through plans A-D to solve the problem. The algorithm is thus an active, integral part of the response.
Key concepts in the framework
Unanticipated vs anticipated difficult airway
The framework is specifically designed for addressing an unanticipated difficult air-way. Suspicion of a difficult airway should prompt planning for the intervention, such as delivery or operation, to happen in a centre experienced in managing the difficult airway. Other times of potential risk, such as planned intubation or extubation of apparently well neonates in non-specialist centres, should prompt planning for what will be done if the process fails.
When to declare the difficult airway
A difficult airway may be defined as: “…a clinical situation in which a trained practitioner experiences difficulty with face mask ventilation, difficulty with tracheal intubation, or both.”5 It is not uncommon in neonatal practice for inexperienced clinicians to be offered the opportunity to intubate followed sequentially by more senior colleagues, up to consultant, with varying degrees of success. The working group consensus for defining the threshold for declaring a difficult airway situation was therefore:
The experienced clinician available varies between settings. The framework acknowledges additional challenges of senior clinicians being off-site out of hours. The aim is to prevent multiple attempts at intubation before considering other options. Specifically, intubation attempts may be abandoned before a set number have been made allowing early consideration of alternative ways forward. Individual centres should assess and set their threshold for declaration, by defining which of their staff meet their acceptable definition of experienced clinician in their own setting.
Front of neck airway (FONA)
Under general anaesthetic an elective tracheostomy is challenging but technically possible in neonates who weigh >1.5kg. In the emergency ‘can’t intubate, can’t oxygenate’ situation, in non-optimal operating conditions, the chances of success even with an expert operator are greatly reduced. If tracheostomy is included in plan D it must only be attempted by appropriately trained, experienced surgical personnel.
In neonates, scalpel cricothyroidotomy is not possible owing to the inadequate size of the cricothyroid membrane and neonatal subglottis. Needle cricothyroid-otomy will neither be successful nor effective in the neonate for the same reasons. FONA is not recommended as an option for the management of a difficult neonatal airway in any setting outside a centre that has an established paediatric ENT surgery service.
Role of neonatal transport teams or regional flying squads
in plans A-D
There is comprehensive UK-wide provision of neonatal intensive care transport. If there is a ‘can’t intubate, can’t oxygenate’ situation there are only minutes to remedy the problem and therefore solutions must be in place inhouse, not including the attendance of a transport team. Similarly, babies cannot be safely transported with mask ventilation as the means of sustaining their airway. A secured airway is necessary for safe transport.
Drugs and the difficult airway
Teams should have agreed protocols for which medicines, if any, they will use in the context of the difficult airway. In principle, medicines chosen should be easily administered, quick acting to achieve adequate sedation and paralysis, and either short-acting or reversible. Staff must ensure familiarity with using any medicine chosen.
Adequate doses of muscle relaxants will ensure paralysis, optimising intubating conditions with no risk of laryngospasm. Mask ventilation may be made easier by using muscle relaxants. If, however, there is doubt about the ability to maintain mask ventilation after paralysis, muscle relaxants should not be used and spontaneous ventilation maintained.
Where intubation and all other attempts at oxygenation have failed, muscle relaxants should be given if not already used. Paralysis may improve both mask seal and airway adjunct efficiency, resolve laryngospasm, and optimise intubating conditions.
Rarely, administration of muscle relaxant unmasks an anatomically difficult airway, such as tracheal stenosis where spontaneous breathing sustained ventilation through a coexisting tracheooesophageal fistula. While reversing neuromuscular blockade is unlikely to help, allowing the neonate who was breathing effectively before paralysis to spontaneously breathe again may make the situation slightly more stable.
Families
While an unexpected difficult neonatal airway is hugely stressful for the clinical team, it is likely to have also been unexpec-ted and catastrophic for the family. It is essential that wherever possible the clinical team assign an experienced staff member to support the family and communicate progress with them, as well as facilitating them to be present with their baby wherever possible should they so wish.
Summary
The BAPM framework for managing the difficult neonatal airway provides a process that allows any team that looks after neonatal patients to organise a cohesive, multidisciplinary contingency plan, which can then be activated in response to the emergency that is a difficult neonatal airway. The role of neonatal airway lead is central to the effective establishment and implementation of this plan, utilising resources outside the normal neonatal environment where needed, and encouraging multispecialty working to optimise the chances of successfully addressing the difficult neonatal airway.
Author contributions
RT drafted the original terms of reference and scope of the Framework with AF. RT chaired the Framework working group and wrote the first draft of this manuscript. Both RT and AF revised this manuscript for final publication.
Acknowledgements
This article draws on the content of the BAPM framework for managing the difficult neonatal airway. The framework, and this article, would not exist without the generous contribution in time, expertise and resources provided by the working group. Thanks for their invaluable input to the working group go to:
Steven Powell, Consultant Paediatric Otolaryngologist; Stephanie Bew, Consultant Paediatric Anaesthetist; Dan Gilpin, Consultant Paediatric Anaesthetist; Jonathan Cusack, Consultant Neonatologist; Ruksana Patel, ANNP; Claire Keeling, Paediatric Specialty Trainee; Matt Thomas, Consultant in Paediatric Respiratory Medicine; David Bartle, Consultant Paediatrician and Neonatal Clinical Lead; Andrew Breeze, Consultant in Obstetrics, Subspecialist in Maternal & Fetal Medicine; Kate Dinwiddy, Chief Executive, BAPM; Helen Mactier, Consultant Neonatologist and President BAPM; Stephen Wardle, Consultant Neonatologist and BAPM Honorary Secretary; Barry McGuire, Consultant Paediatric Anaesthetist; Alok Sharma, Consultant Neonatologist; Carmel Cassar, Consultant Paediatric Anaesthetist; Renuka Arumainathan, Paediatric Anaesthesia Research Fellow; Katie Misselbrook, Anaesthetic Specialty Trainee; Andrew MacLaren, Locum Consultant Neonatologist.
Or read this article in our
Tablet/iPad edition
- The BAPM framework for managing the difficult neonatal airway provides: definition of the role and responsibilities of the neonatal airway lead; a process to optimise resources available in any setting in which a neonate with a difficult airway may present; a pathway for managing the difficult airway to be adapted for local use, which will also be familiar to other specialties that have their own established difficult airway processes; a resource materials document to assist those developing a structured process.
