

Independent prescribing from an ANNP perspective: a reflective analytical case study
This analytical case study reflects on independent prescribing from the perspective of an Advanced Neonatal Nurse Practitioner (ANNP). Focusing on a premature infant admitted to the neonatal unit for intensive care management and monitoring, the article serves to demonstrate prescribing decision-making skills including comprehensive critical analysis and synthesis of the competency dimensions within a competency framework.
Ana GomezAdvanced Neonatal Nurse Practitioner (ANNP), Dyson Unit for Neonatal Care, Royal United Hospital, Bath
anagomez@nhs.net
The Royal Pharmaceutical Society (RPS) Competency Framework for all Prescribers1 outlines and supports effective prescribing for all medical and non-medical prescribers (NMPs). The framework comprises 10 competencies across two domains: consultation and prescribing governance (FIGURE 1). The Nursing and Midwifery Council (NMC) has recently replaced the Standards of Proficiency for Nurse and Midwife Prescribers2 with the RPS competency framework as it underpins the standards of prescribing practice required for all prescribers on the NMC register.3
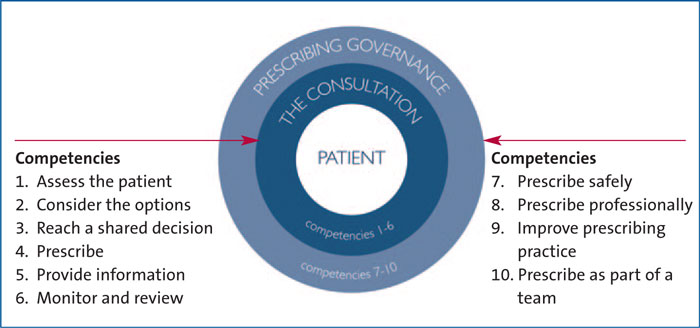
FIGURE 1 The RPS prescribing competency framework (RPS 20161).
This article aims to demonstrate prescribing decision-making skills, including comprehensive critical analysis and synthesis of the competency dimensions within the RPS framework by presenting a reflective analytical case study on independent prescribing from the perspective of an independent and supplementary NMP and focusing on a premature infant admitted to the neonatal unit (NNU).
The case
The case study relates to the assessment and follow-up management of a one-day-old 28+2 weeks’ gestation female infant admitted to the NNU following birth by caesarean section due to a suboptimal fetal heart rate recorded via cardiotocography and concerns regarding maternal chorio-amnionitis. The infant was born in reasonable condition but required intubation in theatre due to respiratory insufficiency. Rescue surfactant was administered via an endotracheal tube, the infant was stabilised and transferred to the NNU for further assessment, management, and monitoring. The infant had a partial septic screen and commenced antibiotic therapy as there was a significant risk of sepsis due to prematurity and maternal infection. Central lines were inserted via the umbilicus in order to deliver total parenteral nutrition. With parental consent, the infant received prophylactic vitamin K to prevent haemorrhagic disease of the newborn. The infant was also loaded with caffeine citrate infusion for the treatment of apnoea of prematurity (AOP). The patient did not have any known drug allergies or sensitivities.
The consultation – competencies 1-6
The neonatal team had discussions with both parents prior to the delivery and both were aware of the management and different levels of support the infant may require depending on condition at birth and postnatal progress within the NNU. Various models of consultation can be found within the literature. While all consultation models include the taking of a medical history, some place more emphasis on the diagnosis of the patient whereas others focus more on the needs of the patient.4 However, all models agree that communication is the cornerstone of the process and that it is important that healthcare providers involved in consul-tations develop strong communication skills.5 Effective communication is essential for all healthcare professionals, particularly in emergency situations within acute clinical areas such as the neonatal intensive care unit in which life is threatened;6 this leads the prescriber to prioritise those aspects of the assessment that should be investigated first.7
One of the key elements of the consultation process is the exploration of ideas, concerns and expectations.8 When initiating a consultation with the parents it is important to establish what they already know in order to build on existing knowledge and correct inaccuracies.5 Furthermore, this approach may also help the family feel that the clinicians are seeking their partnership, rather than simply talking to them.9 In order to establish a rapport with the parents, it is essential to provide appropriate reassurance as well as being aware of the emotions that may be experienced by the family members.10
The relevancy of taking an appropriate medical, social and medication history is clearly detailed in competency 1 of the Competency Framework for all Prescribers. Effective history taking as part of the consultation process is fundamental for safe practice and for preparing to prescribe.11 The assessment represents not only a process of gathering and organising information but also the basis of the therapeutic relationship; hence the communication between the patient and the physician is key to a successful consultation.12 Involving parents early in the decision-making process helps to establish a relationship of trust between the family and the neonatal team, increasing parental satisfaction and compliance with their child’s treatments, and enabling the provision of excellent care that will contribute to the infant’s outcomes.13,9
Although the parents had already been consulted and updated on their infant’s progress by the neonatal team on admission, the birth of a preterm infant can be an intensely stressful and difficult time for parents. The information retained by family members under these circumstances is likely to be minimal and the levels of anxiety, fear and insecurity predicted to be high.14 Furthermore, the communication and interaction process with the parents should be open and continuous and it is therefore important for practitioners to stress their availability if further concerns or questions arise at any point during their journey in the NNU.9
The prescribing decision should be made only after an appropriate clinical assessment.1 This assessment must include accessing patient records to ensure knowledge of the patient’s management to date, and the investigations necessary to inform treatment options.12 Therefore, the relevant information was gathered after the history taking, physical examination and assessment of available tests and included co-morbidities, existing medication, allergies, contraindications and quality of life impacts on management options. Taking into account all the data gathered during the consultation process, the working diagnoses at that point were prematurity, respiratory distress syndrome and significant risk of sepsis.
Recognising the parents as partners in care is the foundation of family-centred care.15,16 For prescribing to be morally as well as professionally sound, the ethical principles of autonomy, non-maleficence, beneficence and justice are also to be considered.12 It is imperative that the physician facilitates open and honest communication with parents in the decision-making process to reach plans that are ethically sound to both professionals and parents.17 In line with competency 2 of the competency framework, both non-pharmacological (including no treatment) and pharmacological approaches to modifying disease and promoting health were considered, applying an understanding of the pharmacological characteristics of the medication selected and how these may be altered. Since the infant had already received a loading dose of caffeine citrate, a maintenance dose of caffeine citrate at 5mg/kg twice a day was proposed.18 Competency 4 indicates that the prescribing decision process should be accomplished within relevant frameworks as local formularies, care pathways, protocols and guidelines. To adhere to this competency the evidence and the protocol of the local trust were reviewed.19
In neonatal medicine, AOP is one of the most common reasons for the initiation of drug therapy, with the administration of caffeine citrate as respiratory stimulant being one of the most frequently prescribed medications.20 Caffeine reduces AOP and decreases the time preterm infants spend ventilated and on supplemental oxygen, leading to less lung damage and less chronic lung disease.21
In line with competencies 3 and 5, the findings of the examination were discussed with the parents and they were informed that their infant would continue to be closely monitored within the intensive care setting due to prematurity. Regarding the proposed medication, parents were notified that the recommended treatment would continue to be monitored and its effectiveness reviewed at ward rounds by the medical team, with potential unwanted effects such as tachycardia constantly observed for (competency 6). With caffeine being one of the most prescribed medications in neonatal medicine,20 providing parents with a leaflet on the use of this treatment would further support consultation and increase parental understanding and engagement with their infant’s care.17 It is important that there is clear documentation around a prescribing decision (competency 4). The patient consultation and detailed summary of findings and prescribing decision as well as plan of action were timely documented on the patient’s medical notes, enabling other professionals involved in the patient’s care access to this information. It was also documented that the parents were updated and involved in the plan of care of their infant.
Prescribing governance – competencies 7-10
Competency 7 establishes that the prescriber should act within their own scope of practice, being aware of the limits of their own knowledge and skill. The original prescription was written by the consultant due to the author not being able to issue a prescription as not yet a registered prescriber. However, the prescription was written by the author as part of a prescribing log ensuring confidence and competence to prescribe were maintained (competency 8). Furthermore, and in line with competency 9 of the framework, the author pursued feedback from the consultant and later reflected on their own practice and overall performance in order to improve skills to become a safe and competent prescriber. The importance of reflective practice for decision making is highlighted by Ellis22 as it allows NMPs in-training to consider what has been successful and what could be improved for future practice. The prescription was written working within clinical governance frameworks that include the audit of prescribing practice and personal development. Although the rest of the trust now uses electronic patient records, paediatrics continues to use paper charts at present. Prescribers should continue to be vigilant as there seem to be more errors on paper charts compared to electronic prescribing.23
Afseth and Paterson24 recognise that collaboration is needed between different health professionals in order to make safe and effective prescribing decisions. To guarantee a safe and prompt administration of the proposed drug to the patient, the named nurse responsible for the care of the infant was informed in a timely manner about the written prescription. It was also ensured that support and advice to those involved in the administration of medicines were provided (competency 10).
It was proposed that the medication would be prescribed within the role of the NMP and in this particular case as an independent prescriber. The development of non-medical prescribing within the health service enables suitably trained healthcare professionals to enhance their roles and effectively use their skills and competencies to improve patient care in a range of settings, as well as making it easier and quicker for patients to get the medicines they need and increasing patient choice in accessing medicines.25 There are two types of NMPs (TABLE 1):
- Supplementary prescribing – a voluntary partnership between an independent prescriber (doctor or dentist) and a supplementary prescriber to implement an agreed patient-specific clinical management plan (CMP) with the patient’s agreement.26
- Independent prescribing – prescribing by a practitioner that is responsible and accountable for the assessment of patients with undiagnosed or diagnosed conditions and for decisions about the clinical management required, including prescribing.25
These definitions are clearly underpinned by legal, professional and ethical principles.
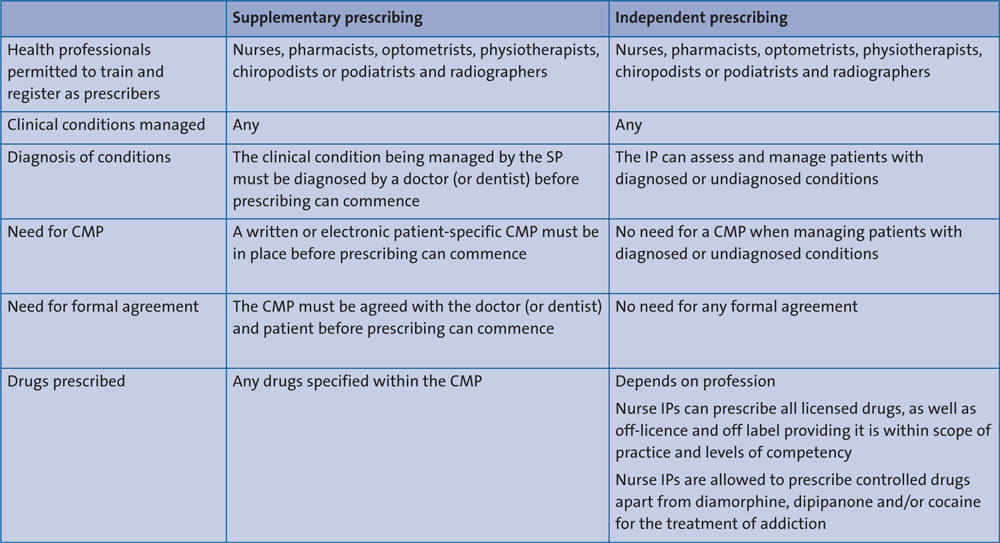
TABLE 1 Supplementary and independent prescribing. Key: CMP= clinical management plan, SP= supplementary prescriber, IP=independent prescriber.
Accountability is a key element of non-medical prescribing; all registered NMPs are personally accountable for their practice and when prescribing must work to the same standards and competence that applies to all other prescribers.27 Furthermore, NMPs are required to work within the boundaries of their own standards of conduct with the intention
of providing high-quality standards of health care, safeguarding the public and promoting professional credibility.28 An independent prescriber (IP) is accountable in four areas of the law and can be held to account under any/all of these areas:
- Legal – this element forms part of professional responsibility and accountability for the protection of the public.
- Professional responsibilities are defined by a duty of care to users, professional codes of conduct and in some cases, state registration and regulation.
- Employment – employee responsibilities are defined by a contract of employment, which usually includes a job description setting out responsibilities in detail. In doing so, IPs are covered by employers’ vicarious liability, making the employer indirectly responsible for the actions of the IP in carrying out their contracted duties.29
- Ethical responsibility.
Conclusion
The prescribing decision process involves a comprehensive assessment of the patient in which the NMP should gather all the relevant information in order to establish a working diagnosis that leads them to consider the treatment options and discuss these with the patient/parents/carers before prescribing a pharmacological treatment. Therefore, at the time of writing the prescription the prescriber should be aware of the clinical situation of the patient and the pharmacological characteristics of the medication. The prescriber must explore the understanding and concerns of the patient/parents/carers about the treatment and have a plan in place to monitor and review the response regarding the treatment and the potential adverse drug reactions that could occur.
The multi-professional competency framework recognises that a common set of competencies underpins all prescribing across the professions, allowing prescribers to deliver a safe and effective prescribing intervention.
Prescribing decision making is a key skill for all prescribers. It is one of the cornerstones of patient safety and it can be challenging. However, experience in the role, peer support and the use of evidence-based guidelines will help in ensuring future safe, effective and optimal prescribing decisions that will enable the future prescriber to master the art of consultation through clinical practice, close supervision and personal reflection.
Or read this article in our
Tablet/iPad edition
- The prescribing decision process involves a comprehensive assessment of the patient leading to consideration of treatment options and discussion with the patient/parents/carers prior to prescription of a pharmacological treatment.
- The Competency Framework for all Prescribers recognises a common set of competencies underpinning all prescribing and providing consistency across professions.
