

Nutritional intake of preterm infants – an audit of practice at a tertiary neonatal unit in Scotland
Optimal early nutrition leads to better long-term outcomes for premature infants. Preterm neonates, especially those born at less than 30 weeks’ gestation, require parenteral nutrition to meet their high energy and protein requirements. Neonatal units have a responsibility to ensure they are delivering the best possible care by comparing their practice with existing standards. We present a clinical audit performed at the neonatal unit of Princess Royal Maternity Hospital, Glasgow, on nutritional intake in preterm infants over the first two weeks of life.
Asma YasmeenConsultant Neonatologist, Victoria Hospital, Kirkcaldy. Previously Princess Royal Maternity Hospital, Glasgow
asma.yasmeen@nhs.scot
Andrew MacDonald
Paediatric Trainee, West of Scotland
Gregor Scott
Paediatric Trainee, West of Scotland
Muhammad Bilal Saqib
Statistical expertise
University of Lahore, Pakistan
Setting: Princess Royal Maternity Hospital, Glasgow
Provision of parenteral nutrition (PN) is an important aspect of neonatal care for premature infants. It provides energy, carbohydrates, proteins, essential fatty acids, minerals, vitamins and trace elements. PN is administered by intravenous route and can be used as the sole source of nutrition (total PN/TPN) or to supplement enteral milk feeds (partial PN). The relationship between optimal protein and energy intake during the first week of life is associated with better neurodevelopmental outcomes at 18 months of age in extremely low birth weight infants (<1,000g).1
Growth of preterm infants in neonatal intensive care units is affected by nutritional and non-nutritional factors (such as inflammation/infection, etc). The physical growth parameters of premature infants lag behind the reference fetal growth parameters indicating compar-atively reduced accretion of nutrients, which may affect brain development.2 In a longitudinal UK population study looking at the growth of preterm infants less than 32 weeks’ gestation at birth, it was found that the mean weight dropped by at least two centiles.3 Poor growth was also noted in the EPICure study cohort in their early childhood.4 Hence, it is very important to focus on early nutritional management in order to improve long-term growth as well as developmental outcomes.
The British Association for Perinatal Medicine (BAPM) framework (2016)5 provides indications and standards for PN formulations along with recommendations for intake of energy and protein. Similarly the European Society for Paediatric Gastroenterology, Hepatology and Nutrition (ESPGHAN) published a set of criteria for adequate energy and protein intake in 2010.6 Since carrying out our audit, ESPGHAN has revised its guidelines7,8 and in addition, the National Institute for Health and Care Excellence (NICE) published a clinical guideline for neonatal PN.9 Protein is required for lean mass accretion. If an optimal amount of energy is not provided, proteins/amino acids will be used as an energy source and this will, therefore, limit growth. The standards for total energy intake include protein as well as carbohydrates and lipids; however, the majority of energy should come from non-nitrogenous sources (ie from carbohydrate and/or lipid) in order to spare the proteins for tissue repair and new tissue deposition. Energy requirements are slightly less in preterm infants on TPN, compared to enterally-fed infants since the intestine is bypassed.
The clinical audit
The clinical audit presented here was performed at the neonatal unit of Princess Royal Maternity Hospital (PRMH), Glasgow, on preterm babies <30 weeks’ birth gestation over the first two weeks of life. We included infants born at less than 30 weeks’ gestation admitted to the neonatal unit at PRMH over an 18-month period between 1 January 2018 and 30 June 2019. We excluded infants born elsewhere, transferred out at less than one month of age, those that died or had necrotising enterocolitis, critical illness, or major congenital/chromosomal abnormalities.
Aims
The aims of the audit were to:
- Measure energy and protein intake during the first two weeks of life and compare with BAPM 201655 and ESPGHAN standards 2010.6 (TABLES 1 and 2).
- Compare ‘z score’ for weight at birth and 36 weeks’ corrected gestation.
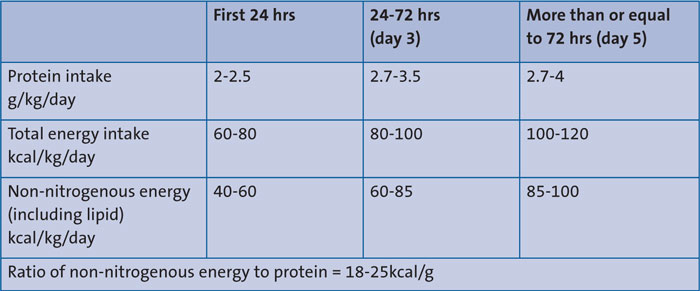
TABLE 1 BAPM 2016 standards.
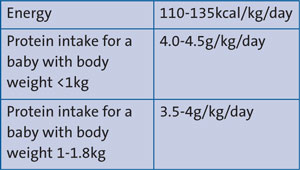
TABLE 2 ESPGHAN 2010 standards.
Z score is used to accurately assess and monitor growth parameters such as weight, head circumference and length/height. The z score is the standard deviation above or below the mean. A z score of 0 corresponds to the 50th percentile; z score of -1 plots at the 16th centile, and +1 corresponds to the 84th percentile. The change/difference in the z score over a time interval (from birth to 36 weeks’ corrected), if negative, indicates that the infant has fallen off their birth centile even if they are gaining weight on a lower growth centile.10
Methods
Data collection
Data were collected from case notes and online patient databases. Z scores were taken from iGrow, an online patient database for recording growth.
PN types
Standard aqueous PN with protein of 2.6g/100mL (and 10% dextrose base) used in 29 babies. One infant received concentrated PN (protein 3.5g/100mL, 16.8% dextrose base).
Lipid formulation types
We used either:
- Intralipid 20%
- Vitlipid N
- SMOFlipid 20%.
Milk
Mother’s or donor breast milk or fortified breast milk was used during the first two weeks.
Results
Out of 75 infants admitted to the unit at <30 weeks’ gestation during the study duration, 43 met the inclusion criteria. A representative sample was taken (by stratified random sampling) for study with 37% infants born at 23-26 weeks’ and 63% born at 27-29 weeks’ gestation.
There were 12 females and 18 males. There were 15 infants weighing <1kg and 15 weighing between 1-1.8kg. All infants were started on PN on day 1. Lipid infusion was started in 23 (76%) babies on day 1. All infants received lipids on their second day of life.
Protein
The median protein intake was found to be lower than BAPM and ESPGHAN standards on day 1, day 3 and day 5 (TABLE 3). On a detailed review of protein intake from day 3 to day 14, infants met the BAPM standard on 55% of the days (median 2.77g/kg/day; mean 2.74g/kg/day). The protein intake from day 3 to day 14 in the <1kg and 1-1.8kg groups, did not meet the ESPGHAN 2010 criteria on 99.5% and 94.5% of days, respectively. The median cumulative protein balance during week 1 and week 2 was 16.7 and 20.1g/kg/week, respectively.
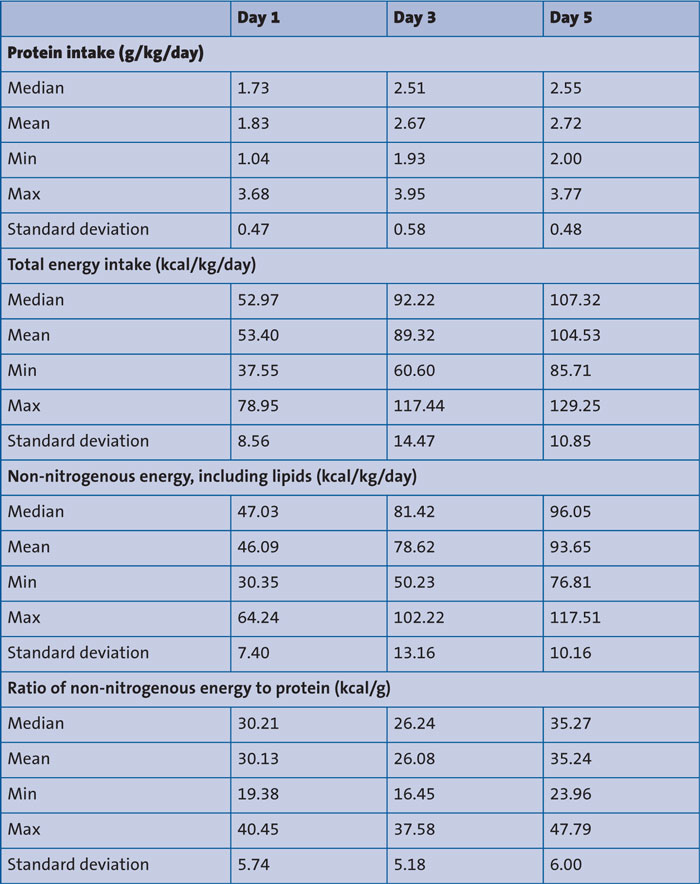
TABLE 3 Audit results showing protein intake, total energy intake, non-nitrogenous energy (including lipids) and ratio of non-nitrogenous energy to protein.
Energy
The total energy intake on day 1 was less than the BAPM standard (median 52.9kcal/kg/day). On day 3 and day 5, the median energy intake was 92-107kcal/kg/day (TABLE 3), thus meeting the BAPM standards. The median non-nitrogenous energy and ratio of non-nitrogenous energy to protein intake met the BAPM standards. The energy standard proposed by ESPGHAN 2010 was not met on 38% of days from day 3 to day 14. The median cumulative energy balance during week 1 and week 2 was 632 and 915kcal/kg/week, respectively.
Z score
The median z score difference between weight at birth and 36 weeks’ corrected age was -1, which indicates that the median weight drop was equal to one standard deviation in the study population. It is well known that existing preterm charts do not adequately describe the pattern of longitudinal growth. Our result reflects similar findings to a UK population-based study by the Neonatal Data Analysis Unit and the Preterm Growth Investigator Group,3 which showed a drop in weight by two centiles for a cohort of preterm babies born at <32 weeks’ gestation. This longitudinal growth pattern could indicate differences in provision of nutrition, greater insensible water loss and/or more illnesses experienced by premature infants. Using individualised growth trajectories could be a better alternative for assessment of longitudinal growth but needs further research and validation.11
Discussion
Overall the results of our audit showed suboptimal protein intake in the unit when compared with BAPM 2016 and ESPGHAN 2010 guidelines. On day 1, it was partly due to the time spent in securing the umbilical venous line. The protein content of our PN formulation was inadequate to meet the standards.
Comparison with recent standards
Since carrying out the audit, we have compared our results to more recent and updated guidelines. In 2018 (after we commenced our audit) ESPGHAN, along with the European Society for Clinical Nutrition and Metabolism (ESPEN) and the European Society for Paediatric Research (ESPR), published revised joint guidelines on paediatric PN.7,8 In addition, NICE published clinical guidelines for neonatal PN at the start of 2020.9 The energy and amino acid standards set by these frameworks were less than the BAPM 2016 and EPGHAN 2010 standards. These recent changes in energy requirements are derived from the 2004 Food and Agriculture Organization of the United Nations, World Health Organization and United Nations University FAO/WHO/UNU recommendations.12 Due to advances in techniques for assessing body composition, deposition of protein, fat and energy required per gram of weight in the first three months of life, the energy requirements proposed were much lower than the 1985 FAO/WHO/UNU report.13 Thresholds for amino acid requirement for preterm babies were also altered in line with more recent studies on amino acid intake and growth, thus trying to avoid the risk of negative nitrogen balance, ensuring better growth in babies who may or may not be progressing well with enteral feeds and avoiding the potential side effects of excessive intake (eg acidosis, high serum urea, hypercalcaemia or hypophosphataemia, hypokalaemia and refeeding syndrome).9
NICE 2020 recommends caloric intake of 40-60kcal/kg/day on day 1, which is gradually increased (over four days) to a maintenance range of 75-120kcal/kg/day.9 ESPGHAN/ESPEN/ESPR 2018 recommends energy intake on day 1 of at least 45-55kcal/kg/day; later increased to 90-120kcal/kg/day.7 Our results showed that median and mean energy intake on day 1 and days 3-14 met both NICE 2020 (FIGURE 1) and ESPGHAN/ESPEN/ESPR 2018 recommendations (for day 1 and then maintenance energy).
NICE 2020 recommends amino acid provision of 1.5-2g/kg/day on day 1, gradually increased over the next 3-4 days to a maintenance dose of 3-4g/kg/day.9 ESPGHAN/ESPEN/ESPR 2018 recommends amino acid intake on day 1 of at least 1.5-2.5g/kg/day and from day 2 onwards, 2.5-3.5g/kg/day along with non-protein energy of >65kcal/kg/day.8 Our data on day 1 (amino acid intake: median 1.94g/kg; mean 2.05g/kg) and subsequent days met the amino acid requirements recommended by NICE 2020 and ESPGHAN/ESPEN/ESPR 2018 (FIGURE 2). Non-protein energy intake on day 3 and beyond also met the ESPGHAN/ESPEN/ESPR 2018 standard (TABLE 4).
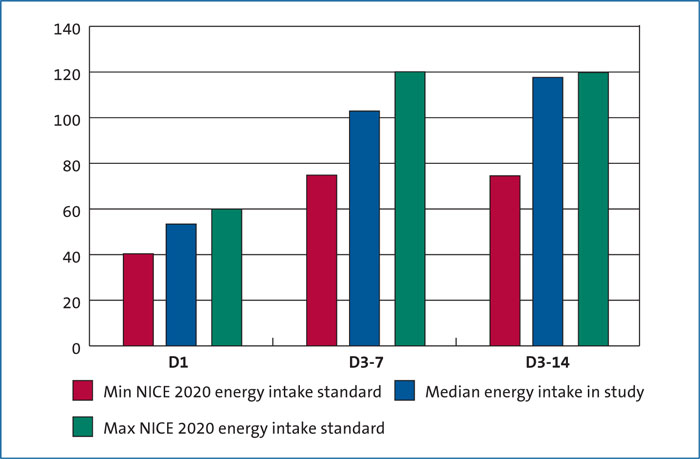
FIGURE 1 Energy intake (kcal/kg/day): comparison with NICE 2020 standards.
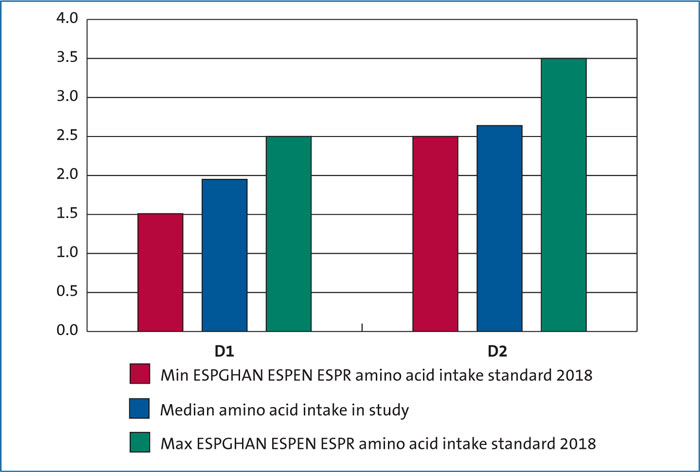
FIGURE 2 Amino acid intake (g/kg/day): comparison with ESPGHAN/ESPEN/ESPR 2018 standards.
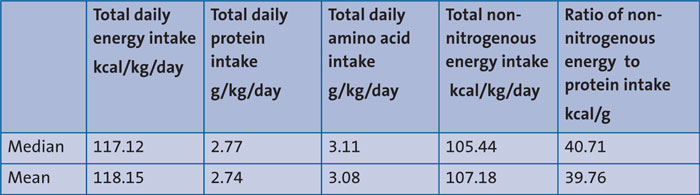
TABLE 4 A summary of nutritional intake on days 3-14.
Recommendations and a re-audit
The current regimen satisfies both NICE and ESPGHAN recommendations. Units using different PN formulations and not meeting the standards could benefit from similar PN formulations. We start lipids and PN soon after birth on day 1 and highly recommend this practice. The introduction of early feeds and the use of fortifier and protein supplements once on full feeds should be considered.
The West of Scotland Managed Clinical Network Guidelines are being revised to be in line with NICE recommendations. One consideration is to commence PN and lipids on day 1 with a 10% dextrose base/sodium-free PN that could be given via a peripheral cannula in babies at 28 weeks’ gestation and above. For smaller gestation babies where central lines are sited routinely, concentrated PN will be used as preference. A future re-audit will be performed 6-9 months after implementation of the new regional guidelines.
Acknowledgement
Special thanks to Pharmacist June Grant for providing details about PN and lipid formulations.
Or read this article in our
Tablet/iPad edition
- The main aim of the audit was to measure energy and protein intake from PN and feeds during the first two weeks of life in preterm babies born at <30 weeks’ gestation.
- Data collected are compared to existing standards, (ie BAPM, ESPGHAN and NICE) to determine if we are adequately meeting energy and protein intake requirements for our babies.
