

Can we do better? Procedural pain relief in neonates: a quality improvement initiative
Procedural pain in neonates has an immediate short-term effect causing physiological instability and may also result in altered pain thresholds and impact on the neurodevelopmental outcomes of an infant over the long term.1,2 Therefore, provision of procedural pain relief in neonates is of vital importance.
Tayyaba YasmeenPaediatric Trainee, West of Scotland
tayyaba.yasmeen@ggc.scot.nhs.uk
Sheena Kinmond
Neonatal consultant, Neonatal Unit Lead
Marie McNairney
Senior Charge Midwife with interest in QI
Caroline Blake
Clinical Midwife Manager Neonatal and Maternity In Patient Services
Ashley Manchester
Midwife
Lynn Montgomery
Midwife
Ayrshire Maternity Unit, NHS Ayrshire and Arran
Background
The historical misconception that neonates are incapable of perceiving pain was still prevalent even until the late 20th century. Now, it is well established that newborn infants can detect, process and respond to painful stimuli.3,4 Studies in preterm babies suggest that they do have the required neuronal connections to experience the affective components of pain:5
- infants as young as 25 weeks’ gestation have been shown to have cortical responses to noxious stimuli
- babies from 28-36 weeks’ gestation undergoing tactile, non-noxious and painful stimuli (venepuncture) display bilateral somatosensory cortical activation following unilateral stimulation.
Preterm infants are more hypersensitive to pain and at greater risk of the detrimental effects of pain due to immature pain inhibition mechanisms at birth.1 Excessive, prolonged painful events in the neonate cause adverse physiological effects in all major organ systems, which can be life-threatening and have long-term impact on neurodevelopment including cognitive development, alterations in brain structure, behaviour, and cognitive ability.6 These differences have been reported in school-aged children, persisting into adulthood.2 Despite the evidence, neonatal pain continues to be inconsistently assessed and inadequately managed. A French study found that only half of painful procedures performed in neonates were accompanied by analgesic therapy, with wide variation in practice.7 Gaps exist in knowledge, evidence and practice of neonatal pain assessment and management, which may be why there are challenges associated with it.
Aims
We set out to improve the frequency of pain and comfort relief measures used in neonates during minor painful procedures, for example heel prick, venepuncture and cannulation.
This quality improvement (QI) project was performed in the level 2 neonatal unit at Ayrshire Maternity Unit (AMU), Scotland. The pain relief measures included breast milk, breast feeding and use of oral sucrose. Swaddling/tucking, non-nutritive sucking and kangaroo care were used for comfort. The West of Scotland guidelines for procedural pain relief in neonates8 and Cochrane’s guidance9-11 were used as standard.
Defining the problem
The guidance on pain relief was not being consistently followed in clinical practice. We identified the problems, developed a project charter and a project team. Baseline data were collected by procedure log sheets over a four-week period (7 October to 6 November 2019). The log sheets recorded:
- Date of procedure
- Patient’s name
- Gestation at birth
- Type of procedure? Heel prick, venepuncture, cannulation
- Comfort/pain relief measure used? Yes/no
- If yes, which comfort/pain relief measure? Swaddling/tucking; non-nutritive sucking; kangaroo care; breastfeeding; breast milk; oral sucrose only; oral sucrose + non-nutritive sucking
- Was the procedure pre-planned? Yes/no
- Were the parents involved in providing pain/comfort relief? Yes/no
- Was assistance available (if needed) to help provide pain/comfort relief? Yes/no
- Any comments/feedback (please specify any barriers to the use of pain/comfort relief)
A total of 85 minor procedures were documented in 22 babies with median gestational age of 34 weeks. During these minor painful procedures, only 62% of babies received pain relief (4.7% breast milk/feeding; 57.6% sucrose) and 48% of babies received comfort relief (15% swaddling/tucking; 25% non-nutritive sucking; 1% kangaroo care; 7% combined swaddling/tucking/non-nutritive sucking). We aimed to increase compliance to 80% for pain and comfort relief measures by the start of March 2020.
Staff and parent survey questionnaires (FIGURES 1 and 2) were used to assess knowledge and current practice and to get feedback about the barriers and areas for improvement. A total of 49 staff members (medical, nursing/midwifery) and six parents partici-pated. The staff survey results showed that 9% of staff felt that babies of <28 weeks’ gestation do not feel pain. Also, 25% of staff surveyed said no/not sure when asked if breast milk/breastfeeding could be used for pain relief. About 33% answered no/not sure when asked if pain has any impact on neurodevelopmental outcomes. More than half of staff felt that giving sucrose in therapeutic doses prior to checking blood sugar levels could alter the results and this was why they avoided using it prior to this common procedure (this is not true). These results highlight misconceptions, hesitation and a lack of knowledge about the use of pain and comfort relief in babies during routine minor procedures.
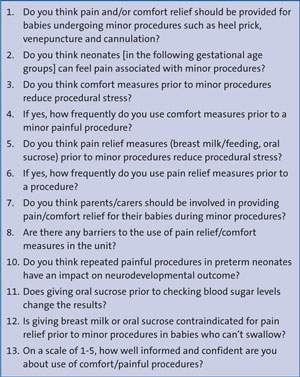
FIGURE 1 Some example questions from the pre- and post-education survey of staff.
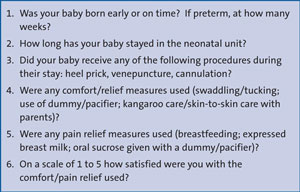
FIGURE 2 The questionnaire for parents regarding pain relief for babies at AMU (note, the actual questionnaire was written in appropriate plain English to ensure understanding).
We used process mapping (FIGURE 3) and fish bone diagrams (FIGURE 4) to highlight the main problems and generate a ‘drivers for change’ diagram describing the aims of the QI project, the primary and secondary drivers and our change ideas (FIGURE 5).
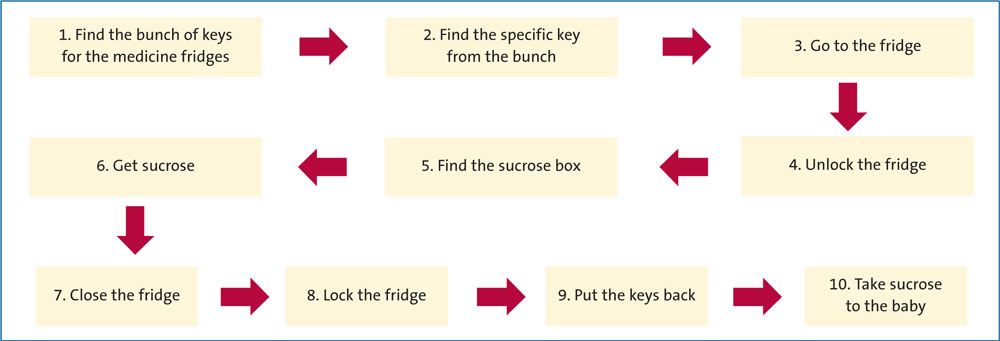
FIGURE 3 An example of process mapping: oral sucrose administration in the neonatal unit.
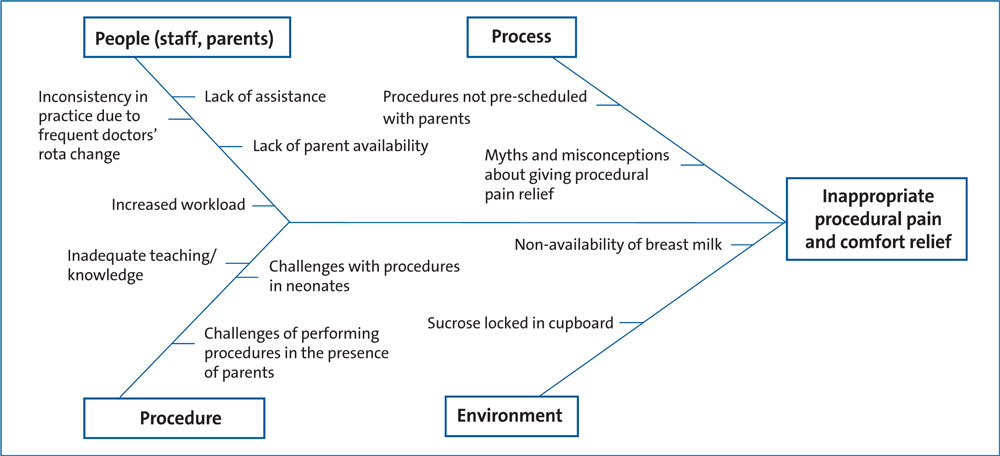
FIGURE 4 A fishbone diagram to clarify why infants were not receiving appropriate procedural pain and comfort relief.
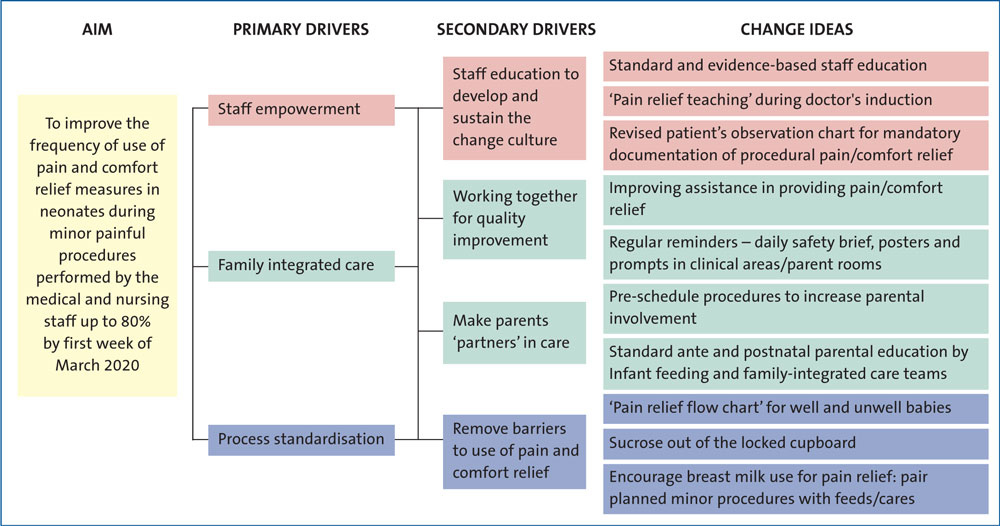
FIGURE 5 The driver diagram for improving the frequency of pain and comfort relief measures at AMU.
Methodology
We discussed the project charter and the improvement plan at the local QI and family-integrated care forums. We educated staff and parents on the rationale of the QI project and how we would implement changes via one-to-one, small and large group teaching sessions for all staff including nurses, midwives, advanced nurse practitioners and doctors, and bedside parental education and formal parental counselling through family-integrated and infant feeding teams. For staff guidance, we developed a pain and comfort relief flow chart for well and unwell babies. We relocated sucrose from the locked cupboard to procedure trolleys for ease of access. We continued plotting the data for use of pain and comfort relief measures on run charts. We conducted two ‘plan, do, study, act’ (PDSA) cycles (FIGURE 6) to consider:
- What are we trying to accomplish?
- How will we know that a change is an improvement?
- What changes can we make that will result in improvement?
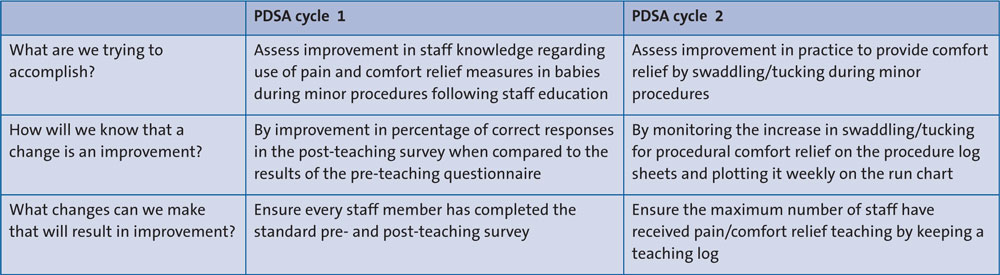
FIGURE 6 The two PDSA cycles.
PDSA cycle 1
Plan:
- pre- and post-education survey questionnaires completed appropriately by staff members
- update staff list to keep a record of the staff who have received the teaching and completed both survey questionnaires
Do:
- compare staff responses in both pre- and post-surveys, review data from all the surveys collected in six weeks’ time; identify areas for improvement
Study:
- on a review of the data we observed a significant improvement in staff knowledge following the staff teaching session
- we identified challenges in coordinating staff teaching sessions without compromising patient care
Act:
- continue to educate staff that haven’t yet attended a teaching session. Encourage other team members to liaise with and facilitate these staff members
- train the trainers: encourage staff who have received the teaching to volunteer to teach other staff members
- review the weekly data in four weeks’ time.
PDSA cycle 2
Plan:
- further staff education
Do:
- collect data on the procedure log sheets and plot it on the run chart to see any trends
Study:
- on a review of the data we observed an improving trend in the use of swaddling/tucking for procedural comfort relief
- it was noted that due to low stock of procedure log sheets, some data were not documented
Act:
- continue to educate staff who haven’t yet attended a teaching session
- provide regular reminders to staff by mentioning procedural pain relief/comfort measures in the morning safety brief and using prompts in the clinical areas
- speak to the ward clerks to ensure procedure log sheets are in good stock.
Measures
Following the introduction of the changes, we collected data on procedure log sheets and used the data to plot weekly run charts to monitor any improvement in practice (FIGURE 7). Data were collected over a period of 15 weeks (27 November 2019 to 7 March 2020) and comprised 180 procedures performed on 54 babies.
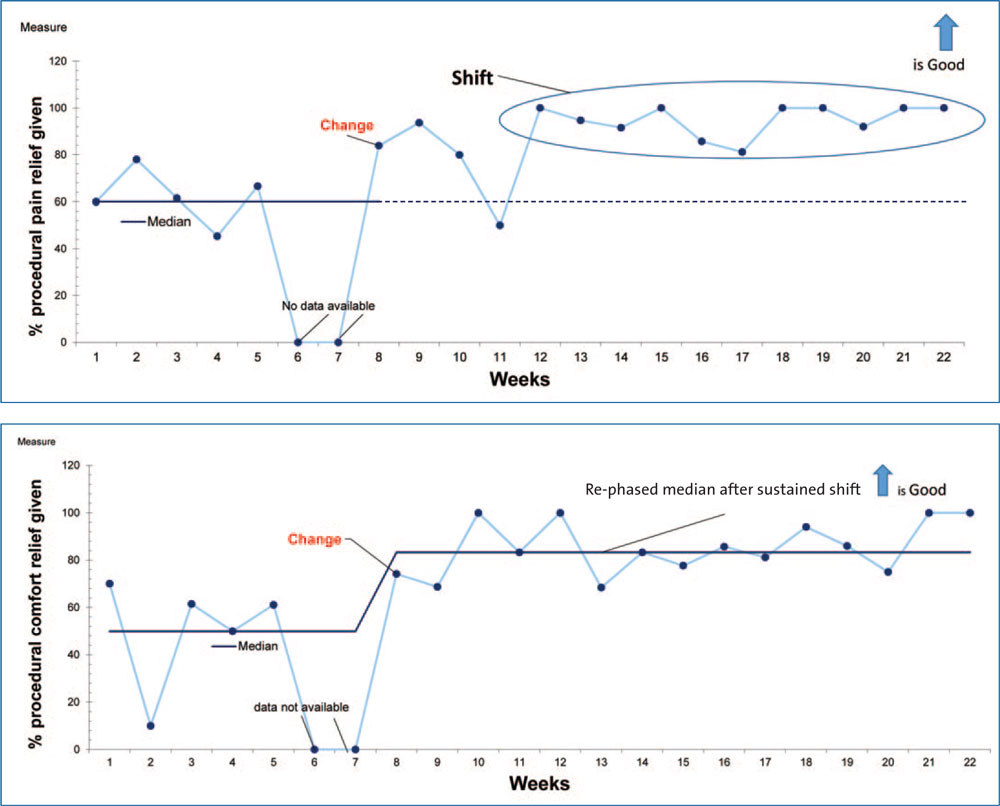
FIGURE 7 Run charts for monitoring improvement in practice. Top: procedural pain relief. Bottom: procedural comfort relief.
We found that there was a ‘shift’ in the use of procedural pain relief and a ‘sustained shift’ in the use of comfort relief measures, as demonstrated in the run charts (FIGURE 7). There was also a shift in the use of individual measures such as oral sucrose, swaddling/tucking, non-nutritive sucking and the use of assistance during procedures. There was a noticeable improvement in assistance by other staff and parents to provide pain/comfort relief during the procedures. As evident in the run charts, our aim to improve pain and comfort relief coverage to 80% was achieved.
Discussion
The importance of the use of procedural pain and comfort relief measures for neonates cannot be understated. This relatively short article describes a rather large undertaking to improve the application of procedural pain and comfort relief measures. A QI project can be a daunting task but to overcome this we developed a well-structured process beginning with defining the problem, developing a plan, implementing and testing the changes and then measuring our improvement. Staff and parent education is of vital importance to overcome any barriers in this process. Encouraging the use of breast milk and kangaroo care for pain and comfort relief not only encourages mothers to breastfeed, but also gives them a sense of achievement in contributing towards the alleviation of pain and discomfort in their child. The changes we implemented demonstrated improvement but ensuring that the changes are embedded and sustained in routine practice will require further monitoring.
Or read this article in our
Tablet/iPad edition
