

Adjusting umbilical central lines using echocardiography ultrasound
This study examined the use of ultrasound for adjusting umbilical central lines in the neonatal intensive care unit at Royal Oldham Hospital. The authors compared ultrasound to traditional X-ray procedures and found that ultrasound-guided placement of the umbilical catheter is a quick, safe and effective method that saves considerable time in clinical and nursing management, especially in extremely premature babies.
Michael SammaanMB BCh, MRCPCH
Neonatology Specialty Registrar, North Western Deanery, Health Education England
michael.sammaan@nhs.net
Arunoday Arunoday
MB BS, MRCPCH, PGDip Neonate
Neonatal Consultant
Neonatal Intensive Care Unit, Pennine Acute NHS Trust
Background
Umbilical catheter placement is a neonatal emergency procedure, which, despite standardised techniques, has a wide variation in practice.1 Umbilical venous catheters (UVCs) and umbilical arterial catheters (UACs) are commonly used in neonates for vascular access and should be carefully inserted to avoid anomalous positioning of the catheter tip. If an umbilical catheter is advanced along the wrong route or too far along its intended course, the tip may end up malpositioned where it may cause harm, injury and, in rare cases, death. Traditionally accurate tip placement is assessed by X-ray and, where necessary, repeat X-rays are performed following catheter adjustment to confirm the tip position. However, commonly used methods of catheter insertion cannot adequately measure the insertion length and X-rays cannot always distinguish malpositioned catheters. Additionally, the use of X-rays for catheter tip confirmation is time-consuming, exposes the patient to radiation and involves excessive handling of a sick infant.
Aim and objectives
In clinical settings, the placement of umbilical lines takes a long time during a critical transition period between medical and nursing care. Ultrasound is a reliable and widely used method for the clinical management of sick neonates in an intensive care unit and it has been shown that it can be used to identify the central catheter tip location.2,3 For this project, we wanted to establish a more time-efficient and precise means of assessing the positioning of an umbilical catheter using ultrasound at the bedside to replace the standard use of X-rays.
Methodology
This quality improvement (QI) project compared the use of ultrasound for adjusting umbilical central lines to the standard X-ray procedure. The study was approved by the clinical audit team and conducted in the neonatal intensive care unit (NICU) at Royal Oldham Hospital, part of the Pennine Acute NHS Trust.
There were two aspects to this QI study. The first was a prospective project looking at any infant admitted to Royal Oldham Hospital NICU requiring UVC and/or UAC placement between May and July 2020.
The infants included in the study were those admitted to the NICU and requiring placement of central umbilical catheters, according to our standard protocol. Newborn babies with congenital defects that affect the abdominal wall or intra-abdominal compartment (such as exomphalos, gastroschisis, single umbilical artery, or suspected or confirmed congenital heart disease) were excluded.
The neonatal team comprised six tier 1 doctors, five advanced nurse practitioners and seven tier 2 doctors, who were responsible for inserting the umbilical catheters. The length of the catheter insertion was calculated independently by the placement practitioner with the objective of optimum placement, as per our unit guideline:4
- for the UVC, the tip should lie at the junction of the inferior vena cava and the right atrium
- for the UAC, the tip should lie between the level of the thoracic vertebral bodies T6 and T10.
The practitioner was allowed to decide which of the various methods would be used for determining length, as per the local unit guideline.
Once the operator had finished and while waiting for the X-ray to confirm the position, limited transthoracic echocardiography was performed in which a 6MHz or 12MHz probe was placed over the mid-chest and upper abdomen to identify the inferior vena cava–right atrial junction and to localise the catheter tip position. An image was recorded at this stage. An instruction was given to the operator to adjust the catheter under real-time visualisation; any adjustment needed was performed under ultrasound guidance and a repeat X-ray was carried out to check the position. Due to its enhanced echogenicity, turbulence generated by the injection of a small volume of saline was also used to confirm the central catheter tip position under real-time visualisation.2 All ultrasound scans were conducted by the authors who have experience and training in targeted neonatal echocardiography.
Finally, an X-ray was performed as an additional safety measure and to reassure those who were not familiar with ultrasound images that the catheter was in an optimal position. Care was taken during the procedure to ensure adequate oxygenation and to maintain a suitable temperature for the infant.
The echocardiogram (FIGURE 1) was recorded for comparison. Using X-ray, the clinical team was reassured that the catheter tip was in an optimal location. The ultrasound results were then correl-ated with the X-ray to show the optimal position of the catheter.
In the second part of the study, we retrospectively reviewed the case notes of 19 randomly chosen neonates who were admitted to our unit who required umbilical line placement. We investigated how many X-ray exposures each baby required before the correct position was achieved and the time needed to achieve that by measuring the minutes taken from putting the request on the electronic system until the X-ray was uploaded onto the system. We did not include the interpretation time as it might vary from one practitioner to another.
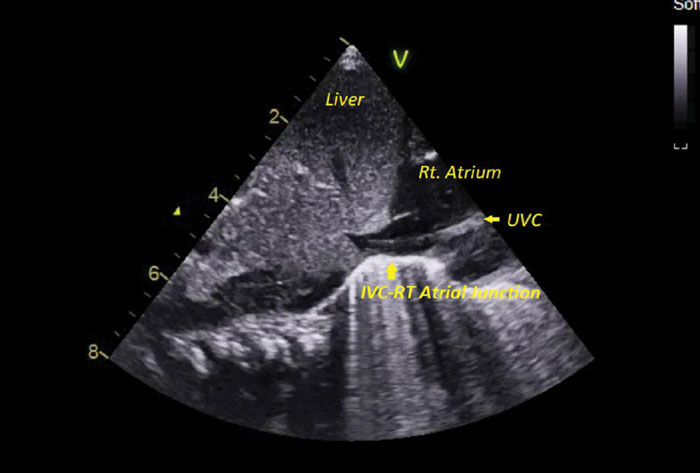
FIGURE 1 Sub-costal view in long axis showing the liver and illustrating the inferior vena cava joining the right atrium and the tip of the UVC 1cm beyond the inferior vena cava–right atrial (IVC-RT atrial) junction.
The outcome measures for this project were:
- the number of X-rays taken
- a time comparison between ultrasound placement versus conventional radiographic placement.
Data analysis and results
A total of 25 infants were enrolled in this QI project. Nineteen infants were randomly selected and their cases were analysed retrospectively. The six infants in the ultrasound-guided group were studied prospectively.
The mean birth weight was 1,910.16g ±1,316.8g (range=790-3,616g) and 1,776.7g ±1,150g (range=413-4,570g) for the ultrasound and conventional groups, respectively (TABLE 1).
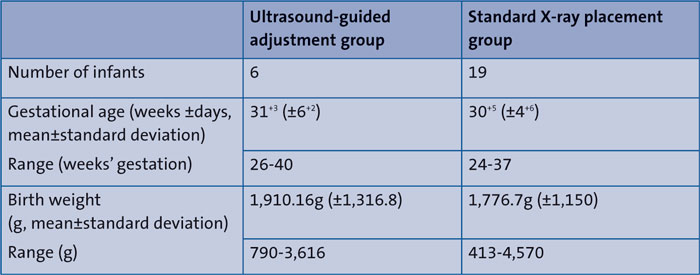
TABLE 1 A comparison of the ultrasound-guided adjustment group with the standard X-ray placement group.
The mean gestational age for the prospective study group was 31+3 (±6+2) weeks (range from 26-40 weeks’ gestation). The mean gestational age for the retro-spective study group was 30+5 (±4+6) (range from 24-37 weeks’ gestation, TABLE 1).
Adjusting umbilical central lines by ultrasound is faster than conventional catheter placement using X-rays. TABLE 2 shows that real-time use of bedside ultrasound decreased the total time of line placement that represented a saving of more than an hour in procedure time.
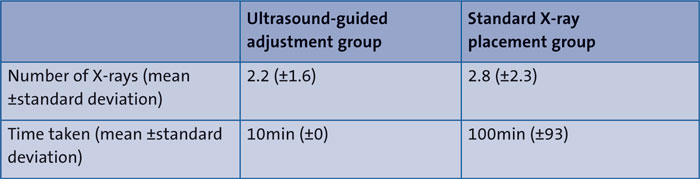
TABLE 2 A summary of the study results.
The average time to acquire and read each series of radiographs was 100 minutes compared to just 10 minutes for correct placement using ultrasound. No manipulation was needed in the ultrasound group following the X-ray; the X-ray was performed as per our unit policy to confirm catheter position for those not confident with interpreting ultrasound images.
With the use of ultrasonic guidance, the catheters required fewer manipulations and X-rays when compared with conventional catheter placement. It was very obvious that it took substantially less time (our estimated time of 10 minutes) to check the position via ultrasound when measuring the time taken from entering the baby’s details into the ultrasound machine to saving the echocardiography clips.
Discussion
In this study, we noticed a substantial difference in the time taken to assess appropriate line placement between the ultrasound and regular placement groups. In the ultrasound group we were able to resume clinical treatment up to 90 minutes ahead of the standard X-ray group due to time saved when requesting an X-ray, alerting the radiographer, taking the films, loading them into a digital system (PACS) and then allowing the doctors to view and interpret the catheter position on the X-ray.
We found that bedside ultrasound was useful both for minimising total procedure time and overall handling during the ‘golden hour’, potentially decreasing the risk of iatrogenic infection, due to reduced catheter manipulation.
In 2019, Meinen5 and colleagues published a review of eight studies that were conducted over the last decade and concluded that point-of-care ultrasound (POCUS) has high sensitivity and specificity in localising the tip of central umbilical lines and is superior to X-ray in terms of reducing time and manipulation in a crucial transitional period.
We recognise that our pilot study was carried out in a small number of babies and involved just two sonographers but we believe that ultrasound-guided placement of umbilical catheters (especially UVCs) can minimise and locate sub-optimal or incorrect catheter placement, hence avoiding catheter-related complications. Furthermore, the speed of ultrasound-guided placement and reduced clinical and nursing handling of the baby, indirectly improves temperature stability with less risk of iatrogenic infection.
Since conducting our study, we have taken steps to train junior doctors in ultrasound-guided catheter insertion with the help of other consultant colleagues who regularly perform in-house echocardiography.
Conclusion
Ultrasound-guided placement of umbilical catheters is more efficient and safer than traditional methods. Through further study and with a greater number of patients, we believe that ultrasound-guided insertion can become the gold standard for placing and confirming umbilical catheters in preterm and critically ill term neonates.
Or read this article in our
Tablet/iPad edition
- Direct visualisation of the umbilical catheter by ultrasound is one of the best modalities for adjusting a UVC and UAC.
- This method can save time needed to help transition a critically ill neonate.
- Ultrasound-guided insertion of a UVC or UAC requires fewer X-rays (hence radiation) and less manipulation and handling of the neonate, helping to maintain temperature and reduce the risk of infection.
