

Congenital enterovirus infection case series: early recognition can improve outcome
Congenital enterovirus infection is caused by a group of single stranded RNA viruses transmitted vertically from an infectious mother; symptoms can begin in utero or in the immediate neonatal period. Symptoms can be mild but when occurring in the first two weeks of life, can be more severe and life threatening. We present a case series of five neonates with congenital enterovirus infection. Three of the infants developed severe infection requiring intensive care, one of whom died of multi-organ failure. A high index of suspicion is required as early treatment may be lifesaving.
Julia ArthurST8 Neonatal GRID Trainee
Sakina Ali
Consultant Neonatologist
Grace Okoye
Consultant Neonatologist
Jean Egyepong
Consultant Neonatologist
Samanthi Mapa
Neonatal Registrar
Fauzia Akhtar
Neonatal Registrar
Rajima Uragaha
Neonatal Registrar
Jogesh Kapadia
Consultant Neonatologist
jogesh.kapadia@ldh.nhs.uk
Neonatal Unit, Luton and Dunstable Hospital
The case series
We reviewed all cases of congenital enterovirus over a 10-year period between December 2009 to December 2019 at the Luton and Dunstable University Hospital NHS Trust’s tertiary neonatal intensive care unit (NICU). Clinical presentation in the first seven days of life was presumed to be congenital. Of the seven infants with neonatal enterovirus infection identified using a database search (BadgerNet), two were excluded as they presented late (day 25 and day 56). TABLE 1 shows the demographic details, mode of delivery, risk factors and whether in-born or out-born.
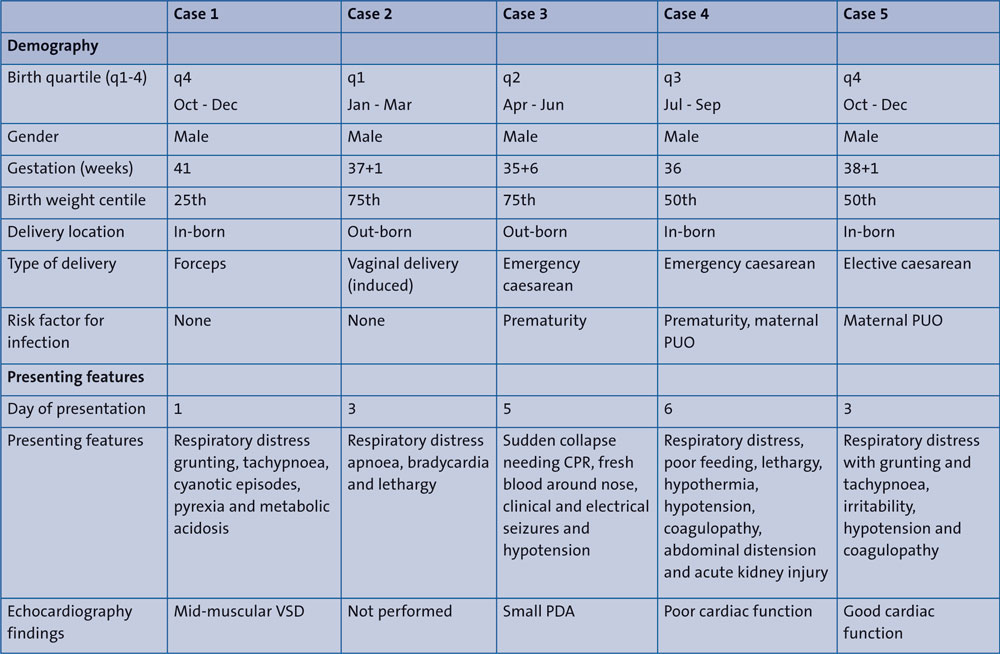
Table 1 Demography, risks factors for infection and presenting features. Key: PUO=pyrexia of unknown origin, CPR=cardiopulmonary resuscitation, VSD=ventricular septal defect, PDA=patent ductus arteriosus.
One case was in 2015, one in 2017 and three were in 2019. The mean age at presentation was 3.6 days (range = 1-6 days). The most common presenting feature was transient respiratory distress. Other associated clinical features included poor feeding and lethargy. Three babies developed hypotension requiring inotropic support, one of whom had evidence of myocardial dysfunction on echocardiogram. Three other babies also had echocardiograms: one had a non-significant patent arterial duct, another had a small restrictive muscular ventricular septal defect, and one was normal. One baby had seizures requiring treatment with anti-epileptics. Two babies developed coagulopathy needing treatment with vitamin K and fresh frozen plasma (FFP) (TABLE 1).
All of the babies had a raised C-reactive protein (CRP, mean = 45.5mg/L) but negative blood cultures. All had a lumbar puncture except one who was deemed too unwell and had thrombocytopenia. Cerebrospinal fluid (CSF) was positive for enterovirus PCR (polymerase chain reaction) in all four of the babies who had the lumbar puncture. Two babies also had enterovirus-positive stool samples and two had enterovirus-positive blood samples. Three of the babies had at least two different samples types sent for enterovirus PCR (TABLE 2). All babies received first line antibiotics (benzylpenicillin and gentamicin) with acyclovir (antiviral drug).
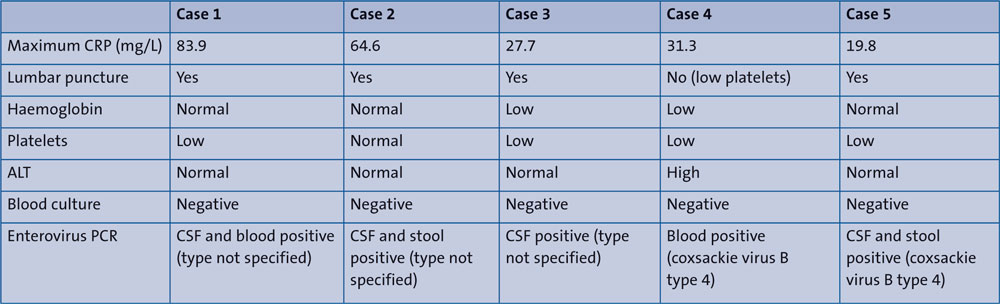
Table 2 Results of investigations. Key: CRP=C-reactive protein, ALT=alanine transaminase, PCR=polymerase chain reaction, CSF=cerebrospinal fluid.
Four babies required mechanical ventilation. Two had associated anaemia requiring blood transfusion and four had thrombocytopenia requiring platelet transfusion. Two infants who required other blood products including FFP, cryoprecipitate and albumin also received intravenous immunoglobulins. Four babies survived to discharge with an average length of stay of 9.75 days. One died of multi-organ failure on day 9 of life (TABLE 3).
Two of our babies who presented with more severe symptoms are described in further detail in the following sections.
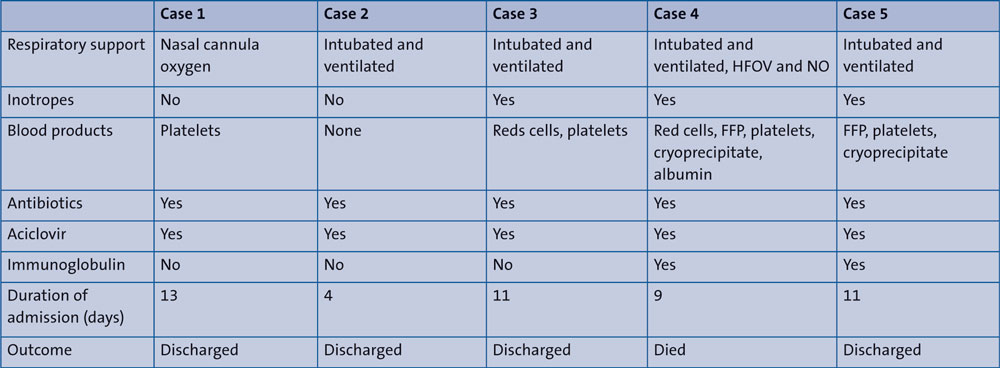
Table 3 Management and outcomes. Key: HFOV=high frequency oscillatory ventilation, NO=nitric oxide, FFP=fresh frozen plasma.
Case 4
The first case to consider in further detail is that of a male infant delivered at 36 weeks’ gestation by emergency section due to fetal tachycardia. His mother had pyrexia of unknown origin for five days prior to delivery, for which she was extensively investigated with blood and urine culture, throat swab, influenza and respiratory syncytial virus PCR, and faeces PCR. All tests were negative except the faeces PCR which subsequently tested positive for enterovirus. She was commenced on cefotaxime and metronidazole initially; the cefotaxime was then changed to meropenem prior to delivery.
The baby was born in good condition and was screened for early onset neonatal sepsis and started on first line antibiotics due to risk factors for sepsis, in line with National Institute of Clinical Excellence (NICE) guideline CG149.1 Infection markers and blood cultures were negative, so antibiotics were stopped on day 3. He stayed on the postnatal ward in view of intermittent poor feeding. He was admitted to the NICU on day 6 with poor feeding, lethargy and hypothermia (35.9°C). On admission he had a full septic screen including viral samples and was recommenced on first line antibiotics with aciclovir. Metronidazole was later added due to abdominal concerns. An abdominal X-ray was discussed with surgeons and was thought to show a septic ileus. Blood results showed thrombocytopenia (platelets 23x109/L) with deranged clotting (prothrombin time, PT = 26.1secs; activated partial thromboplastin time, APTT = 83.1secs; international normalised ratio, INR = 2.0; APTT ratio = 1.5), which required multiple platelet transfusions, additional vitamin K doses and FFP. His clinical status quickly deteriorated over the next 48 hours. His work of breathing increased and he eventually required intubation and ventilatory support.
He developed hypotension, which was initially treated with a fluid bolus, but subsequently required inotropic support with dopamine and dobutamine. He went on to require high frequency oscillatory ventilation (HFOV) and a trial of inhaled nitric oxide after an echocardiogram showed an element of pulmonary hypertension. The echocardiogram also showed very poor cardiac contractility and inotropes were changed to adrenaline and noradrenaline in discussion with the cardiology team. His liver function tests on admission were normal but became increasingly deranged (peak alanine transaminase = 266U/L). He became anuric with evidence of acute kidney injury. He also developed evidence of pulmonary haemorrhages (lot of blood via endotracheal tube) and increasing metabolic acidosis requiring sodium bicarbonate corrections.
He was given intravenous immunoglobulin on day 7 due to the clinical deterioration and a high index of suspicion for enterovirus infection. He deteriorated further on day 8, with persistent brady-cardia and desaturations and required full resuscitation including chest compressions, two doses of adrenaline and sodium bicarbonate, but this was unsuccessful. Viral PCR from blood came back as positive for enterovirus (coxsackie virus B type 4). A retrospective maternal sample (stored stool sample) also tested positive on PCR for enterovirus.
Case 5
The second case to consider in further detail is that of a term male infant delivered by emergency caesarean section due to maternal pyrexia (of unknown origin) and suspected sepsis; the mother was on intravenous antibiotics of cefotaxime and metronidazole. Maternal investigations sent included blood and urine culture, herpes simplex virus PCR, genital swab and faecal culture, which were all negative, and faeces PCR, which tested positive for enterovirus after the baby was delivered.
The baby was born in good condition. Following a partial septic screen, he was started on first line antibiotics (benzylpenicillin and gentamicin) in line with NICE recommendations. He remained with his mother on the postnatal ward and was well in the first 36 hours of life. Initial CRP tests were mildly elevated on day 1 (12.5mg/L) and rose to a maximum of 19.8mg/L on day 5. On day 2 he was noted to be irritable with mild tachypnoea and pyrexial, with temperature spikes up to 38.2°C. A lumbar puncture was performed, and cefotaxime was added to the antibiotics. He was kept under close observations in the NICU and within 24 hours CSF-PCR was reported as positive for enterovirus. Subsequent faecal enteroviral PCR was positive as well (coxsackie virus B type 4). On day 3 he had a clinical deterioration with episodic mild peripheral cyanosis, with saturations dropping to 72%, heart rate to 80 beats per minute and respiratory rate to 45 breaths per minute. He had increasing tachypnoea and work of breathing followed by the development of an erythematous macular-papular rash over his trunk and abdomen with peri-umbilical flare and mild abdominal distension. He was therefore intubated and commenced on mechanical ventilation. He had a repeat dose of vitamin K and FFP due to a mildly deranged clotting profile (PT = 13.3secs; APTT = 79.3secs; INR = 1; APTT ratio = 2.8).
Intravenous immunoglobulin was started on day 3 of life in view of the enterovirus and clinical deterioration; this was transfused over 48 hours. He developed hypotension on day 4 and was commenced on dopamine, which he required for 48 hours. He had echocardio-grams on day 4 and day 10, which were normal with good contractility.
In view of low platelets (44x109/L) he had a platelet transfusion on day 4 of life and he also received cryoprecipitate due to a low fibrinogen of 1.58g/L. On day 5 and 6 of life, his platelets dropped again to 33x109/L and 42x109/L, respectively, so he received two more platelet transfusions on those days. Both his troponin-T and D-dimer levels were raised (647.1ng/L and >5000ng/mL, respectively) but steadily normalised prior to discharge.
In total he received a five-day course of cefotaxime, benzylpenicillin and gentamicin; blood cultures were negative. On discharge (day 12) he was bottle feeding on demand with no concerns. His platelets were 74x109/L at discharge and were normal at follow ups. He examined neurologically well on follow up at three months of life.
A review of the literature
What is an enterovirus?
Enteroviruses are a group of small spherical viruses containing single-stranded RNA, associated with several human and mammalian diseases. The main subtypes are poliovirus, echovirus and coxsackie. Serologic studies have distinguished 71 human enterovirus serotypes on the basis of antibody neutralisation tests. The true prevalence of enterovirus infections in the UK is unknown as it is not routinely tested for.
How is enterovirus transmitted?
Congenital enterovirus is transmitted vertically at delivery but can also be transmitted through close contact of infected persons, either asymptomatic or symptomatic. A study on enterovirus transmission looked at infants diagnosed with enterovirus infection and tested the stools of close family members. They found positive results for enterovirus in 64% of asymptomatic family members and 70% of symptomatic family members.2 This highlights the importance of careful hand hygiene around newborn babies.
Symptoms of enterovirus in neonates
Enterovirus infection is seen in neonates, with consequences ranging from asymptomatic infections to severe, life-threatening disease. Common symptoms include fever, irritability, lethargy, poor feeding and a rash. Although most illnesses are mild, severe disease develops in a subset of newborns infected in the first two weeks of life. Severe disease may include sepsis, meningoencephalitis, myocarditis (mainly with coxsackie virus), pneumonia, hepatitis, and/or coagulopathy (mainly with echovirus type 11). Raised alanine transaminase, thrombocytopenia and deranged clotting should rouse suspicion of enterovirus in a baby with clinical signs of sepsis.3 Pleocytosis is also a feature of enterovirus meningitis.4 Substantial mortality rates have been reported, and long-term sequelae may occur among survivors.2
Risk factors for severe congenital enterovirus infection
Risk factors for severe life-threatening disease include absence of neutralising antibody to the infecting serotype, maternal illness in the week prior to, or at delivery, vertical transmission, prematurity, male gender, illness onset within the first few days of life, multi-organ disease, severe hepatitis, positive serum viral culture, and specific infecting serotypes, eg group B coxsackie viruses and echovirus.5
Diagnosis of enterovirus
The mainstay of diagnosis is viral isolation; reverse transcriptase PCR (rt-PCR) in blood or CSF has been demonstrated to be more sensitive than culture. In a recent French study, PCR in blood was more sensitive than CSF and this group concluded that blood PCR for enterovirus should be included in the work up of all febrile neonates to help rationalise antibiotic use. Higher viral loads are associated with infections within the first week and more severe infections.6 Stool sample/rectal swabs have the highest yields (>90%), however these may be positive for up to three weeks post-infection and are therefore not indicative of acute illness. It should also be noted that the routine panel of rt-PCR for enteroviruses does not test for echovirus 11.
When should enterovirus in neonates be suspected?
Diagnosis of enterovirus infection is difficult without laboratory investigations. A high index of suspicion is the key to early diagnosis in neonates. Maternal pyrexia prior to delivery without a known cause and symptomatic babies treated for suspected bacterial infection with negative investigations should raise suspicions. The onset of congenital infection tends to occur in utero or at 1-2 days of life. Retrospective studies looking at CSF PCR have shown that enterovirus is the diagnosis for 12-27% of febrile infants treated for suspected sepsis.7,8 Enterovirus has a seasonal varia-tion with highest prevalence in autumn and summer, with a 78% incidence in June to October, and serotypes vary over time.9 Early lumbar puncture and rapid CSF PCR is essential for correct diagnosis and management. Routine CSF viral screening has been shown to significantly reduce unnecessary antivirals and antibiotics and reduce hospital stay.10
How is enterovirus treated?
Most infections are self-limiting and only require supportive treatment. In severe disease with its associated high mortality rates, immunoglobulins and anti-viral therapy may be reasonable to use although evidence is limited. Very few studies have reviewed the use of immunoglobulin in enterovirus infection in neonates. The only randomised controlled trial (RCT) looking at immunoglobulin use, in 16 neonates with enterovirus, found a moderate boost in serum neutralising antibody titres, subtle clinical benefits and faster cessation of viraemia.11 A retrospective study looking at 67 cases of culture-positive enterovirus infection found that early immunoglobulin within the first three days was independently associated with survival.12 When considering giving immunoglobulins, the dose should be higher than the conventional doses as the amounts of neutralising antibody present in it are low. The recommended dose is 3-5g/kg.
The antiviral drug, Pleconaril, is an investigational agent that inhibits viral attachment to host cell receptors, uncoating and subsequent release of viral RNA into a host cell. Clinical trials have demonstrated benefit in children and adults with enterovirus meningitis and in adults with upper respiratory tract infections caused by picornaviruses (rhinoviruses or enteroviruses).13 An RCT by Abzug et al (2016), showed a faster time to culture and PCR negativity and an increased trend for greater survival in the Pleconaril group but this was not significant.14 Pocapavir, another investigational drug developed to treat polio, has also been used experimentally in a neonate with enterovirus in combination with immunoglobulins with a good outcome.15,16
Extracorporeal membrane oxygenation (ECMO) also has a role in the supportive treatment of enterovirus myocarditis with cardiovascular collapse and should be considered early. Cortina et al (2018), reported outcomes in seven neonates with enterovirus myocarditis requiring ECMO support; four survived with ECMO and three survived to discharge. All three survivors showed complete cardiac recovery at 36 months.17
What is the prognosis?
In the majority of cases, the illness is benign and self-limiting. Mortality is higher in severe infection. 30-50% mortality has been reported in neonates who develop enterovirus myocarditis,18 with 66% of survivors having severe cardiac injury, which may require a heart transplant. Aspartate aminotransferase is a good marker of severity with a peak at three days (>1,000U/L) being associated with worse clinical outcome.6
Enterovirus infection can lead to acute liver failure and there has been a recent case report of two neonates who received liver transplantation after enterovirus infection with 100% survival.19 Enterovirus can also lead to neurological sequelae. Magnetic resonance imaging of the brain should be considered at 4-6 weeks to look for white matter changes.20,21
Discussion/learning points
From our case review, it is evident that congenital enterovirus infection is uncommon. We had five cases over a period of 10 years. However, early recognition is crucial as it can be fatal, especially if associated with myocarditis. Our review supports that early index of suspicion is key to swift diagnosis and effective management. Two of our infants who were critically unwell also had associated coagulopathy and thrombocytopenia. Viral pathology was considered as a differential but blood/CSF samples for viral PCR from our hospital are sent to a reference laboratory and results can take 48-72 hours. Liaising with the laboratory when tests are urgent is therefore vital. It also highlights the importance of close communication with the obstetric team. Mothers of both cases 4 and 5 were under investigation for pyrexia of unknown origin and, although they had had multiple tests including a viral screen, enterovirus had not been specifically looked for.
This review highlights the importance of early echocardiography in infants with suspected enterovirus infection to assess cardiac function, early inotropic support and that early referral to an ECMO centre should be considered if an echocardiogram shows signs of myocarditis and poor cardiac contractility. Unfortunately, case 4 deteriorated too rapidly – before ECMO was considered a treatment option. Finally, although data are limited, immunoglobulins have been shown to improve outcome if given early. In case 4, immunoglobulins were given empirically. In the event of a high index of suspicion for enterovirus without a positive confirmed result, especially with multi-system involvement, high dose immunoglobulins should be given at the earliest point and ideally within the first three days of the illness.
Or read this article in our
Tablet/iPad edition
- The incidence of congenital enterovirus infection in the UK is unknown and is likely to be underdiagnosed.
- Early treatment for babies with multi-organ failure may be lifesaving.
- There is need for increased awareness of presenting symptoms and early testing. Collaboration with obstetrics and microbiology expedites testing in mothers with pyrexia of unknown origin.
