

Management and outcome for babies born with a gastroschisis
Gastroschisis is an abdominal wall defect present at birth and leading to herniation of the viscera. It is a surgical emergency and therefore delivery should occur in an appropriately skilled centre and/or transfer of the infant to the designated neonatal surgical unit should occur within four hours of birth. There is lack of consensus among the surgical community about the preferred method of management. This review describes key outcomes for 132 infants with gastroschisis admitted to our surgical neonatal intensive care unit over a 10-year period.
Sarah Louise WilliamsonRegistrar in Neonatology
sarahlouise.williamson@nhs.net
Louise Lawrence
Specialist Neonatal Surgical Nurse
G. Suren Arul
Consultant Paediatric Surgeon
Shree Vishna Rasiah
Consultant Neonatologist
Birmingham Women’s and Children’s NHS Foundation Trust
Gastroschisis is a congenital anomaly that comprises a paraumbilical abdominal wall defect leading to herniation of the bowel and occasionally other abdominal organs.1 The herniated viscera are not covered by a surrounding membrane as with exomphalos, therefore being exposed to amniotic fluid during pregnancy (FIGURE 1). The condition was first described by Italian pathologist Cesare Taruffi in 1894, the word ‘gastroschisis’ translating to ‘belly cleft’ from ancient Greek.2 However, a case of gastroschisis, collected by John Hunter in approximately 1750 is preserved in the Hunterian museum at the Royal College of Surgeons but was only recognised in 2008.3 The reported prevalence in the UK varies from one in 3,000-8,000 live births, demonstrating an increasing trend over the last few decades.2,4,5 It is well known to have an association with young maternal age and white Caucasian ethnicity.2

FIGURE 1 The loops of bowel without a covering membrane in gastroschisis. Note how the bowel loops are matted together. This is a typical appearance of the bowel and is thought to be related to prolonged contact with the amniotic fluid.
Gastroschisis can be separated into two types, simple and complex gastroschisis.5 Simple gastroschisis has no evidence of associated complications and accounts for 90% of cases.5,6 Complex gastroschisis accounts for the remaining 10% and is associated with presence of intestinal atresia, necrosis or perforation.5 Liver herniation is a rare complication, found in approximately 6% of patients.7 Survival rates now exceed 95% in high income countries (though significantly lower in developing countries), however poorer outcomes are associated with complex gastroschisis.2,8,9
Surgical management aims to reduce the herniated viscera and close the abdominal wall defect. This can be achieved by primary closure or staged reduction.2
Primary closure under general anaesthetic
This is the traditional method of reduction. Primary closure is performed soon after birth and involves general anaesthesia with muscle paralysis allowing the surgeon to reduce the exposed intestine into the abdomen with surgical closure of the abdominal wall defect under surgically sterile conditions. An intensive care bed is often required because the increased abdominal pressure and pain of reduction makes post-operative breathing difficult. Though a technique has been described of performing primary reduction at the bed side without anaesthetic or aseptic conditions, it has largely been abandoned because of the high complication rate.
Simple vs complex gastroschisis
Simple gastroschisis is defined as only the bowel being outside of the abdomen with no other obvious bowel problems such as atresia or perforation – the techniques described in the following sections relate to simple gastroschisis. Complex gastroschisis occurs when there are obvious signs of atresia (bowel blockage), perforation or that the abdominal wall defect has virtually closed compromising the bowel perfusion and development (known as closing gastroschisis). Complex gastroschisis requires a bespoke surgical management plan that may include formation of a stoma and is associated with a significantly higher risk of surgical and medical complications, multiple procedures and a prolonged hospital stay.
Staged reduction
Staged reduction can either be performed in theatre under general anaesthetic or at the bed side.
Sutured silo performed under general anaesthesia
Silo insertion in theatre under general anaesthetic is usually performed when primary reduction has failed because of concerns that the abdomen is too small to accommodate the entire bowel and that if reduced, compartment syndrome would result or ventilation would be severely compromised. In this technique a silo is fashioned from a sheet of silastic or a modified saline bag and is sutured to the abdominal wall fascia (FIGURES 2-4).

FIGURE 2 The bowel loops are placed in a silo bag which is suspended and aimed at slowly reducing the contents in the abdomen over a few days.

FIGURE 3 The bowel loops are almost completely reduced back into the abdomen.

FIGURE 4 Abdominal closure of the defect following reduction of the bowel loops into the abdomen.
Preformed silo insertion at the cot side
Silo insertion at the cot side is performed under aseptic conditions but without general anaesthetic. A preformed silicon bag with a collapsible spring at the base is used. The technique involves carefully placing the bowel inside the bag and then compressing the ring, which is then inserted under the fascial ring. Once inside the abdomen the ring then opens and holds the bag securely in place, it also tends to hold open the fascial defect to allow easier reduction of the bowel. Reduction occurs over a period of days, monitoring the bowel perfusion through the transparent material, followed by closure of the abdominal wall either on the ward using steristrips or in theatre with a sutured closure. The principle is that with gradual reduction the abdomen can slowly expand to accommodate the bowel without compromising the breathing or bowel perfusion. The main advantage of the preformed silo technique is that it can reduce the need for general anaesthesia and a reduction in the risk of compartment syndrome, which in turn reduces the need for post-operative intensive care.
There is currently lack of consensus among the surgical community about the preferred management method.10 A meta-analysis concluded that silo closure is associated with better clinical outcomes compared with primary closure, especially in infants where primary closure is not readily achievable.10 The perceived benefits of using a silo include reduced risk of respiratory compromise and abdominal compartment syndrome.2 Our aim is to share our experience of managing neonates with gastroschisis and their outcomes in the last 10 years.
Clinical pathway following antenatal diagnosis
In the UK, 97% of infants with gastroschisis are diagnosed in the antenatal period.6 All of these infants are closely monitored by the fetal medicine department and the families are offered antenatal counselling with a multi-professional team, including a consultant paediatric surgeon, neonatologist and surgical outreach nurse.
Gastroschisis is a surgical emergency therefore delivery should occur in an appropriately skilled centre, effective communication between departments being essential. Transfer of the infant to the designated neonatal surgical unit should occur within four hours of birth.
At delivery a plastic clamp is placed on the umbilical cord >5cm away from the infant’s abdomen to avoid bowel injury.11 The baby’s legs and abdomen are then placed in a sterile plastic bag. This whole process should be performed quickly due to the risk of hypothermia and fluid loss from the exposed bowel.11 Resuscitation should be initiated as per Newborn Life Support guidance,12 however prolonged mask ventilation should be avoided and intubation performed in a timely manner to avoid gastric distention. A large (size 8-10fr) nasogastric tube should be inserted to empty the stomach, attaching a free drainage bag. It is essential to ascertain whether the stomach is decompressed as failure of this can result in pressure on the mesentery leading to bowel ischaemia. It is also important to check the colour and alignment of the bowel, ensuring it is not twisted. The infant should be nursed on the same side as the defect, which is usually the right, reassessing the perfusion and alignment every 15 minutes and if vascular compromise is suspected, the surgical consultant should be informed immediately.
On admission to the neonatal intensive care unit (NICU), management is focused on fluid balance and replacement of losses. Infants with gastroschisis have a high fluid requirement until the bowel is replaced into the abdomen, therefore continued cardiovascular and fluid re-assessment is essential.11 Intravenous antibiotics should be commenced as per local policy.
On arrival at the neonatal surgical ward the infant will be assessed by a paediatric surgeon, to decide on the appropriate management strategy. The aim is to achieve reduction of the herniated viscera and closure of the abdominal wall, avoiding the development of compartment syndrome or respiratory compromise.
Method
Birmingham Women’s and Children’s Hospital has a 41-bed tertiary NICU, receiving approximately 2,000 admissions per year. It is the regional referral centre for complex congenital abnormalities. Gastroschisis by itself is not an indication to deliver at Birmingham Women’s and Children’s Hospital; however, babies should ideally be delivered in a NICU with experience of the condition.
Results
Reviewing the unit’s data over 10 years (1 April 2009 to 31 March 2019) revealed that 132 infants were admitted with a diagnosis of gastroschisis; on average 13 infants per year (range = 7-20). Infant demographics are outlined in TABLE 1. Mean maternal age at delivery was 23 years (range = 16-26 years). Complex gastroschisis was diagnosed in 15 infants (11%) (TABLE 2).
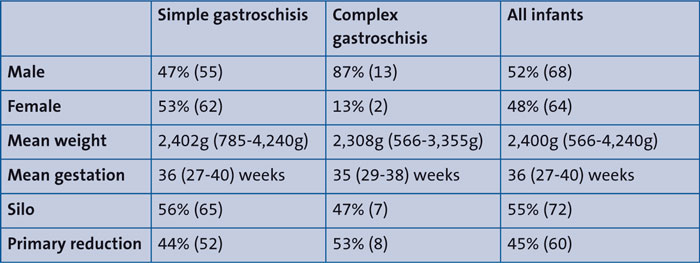
TABLE 1 Infant demographics (n=132).
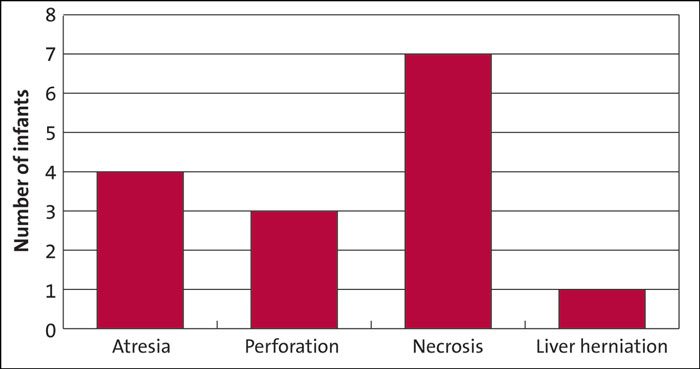
TABLE 2 Complex gastroschisis (n=15) associated with the presence of intestinal atresia, necrosis or perforation. Liver herniation is a rare complication.
Post-delivery, 60 infants (45%) underwent primary closure within the first 24 hours of life. Silo was used as primary management in 72 infants (55%) (TABLE 3). Time to surgical closure in the silo group was on average five days (range = 1-17 days). Stoma formation was required in 11 infants (8%). Six of these infants under-went primary closure (54%). Three of these infants required home parenteral nutrition (2%).
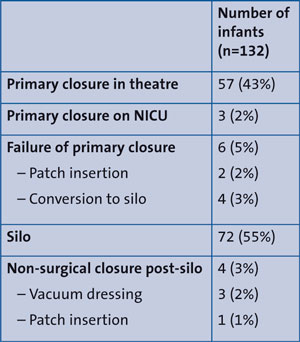
TABLE 3 The closure methods employed.
Overall mortality was 2% (n=3). All infants were documented as complex gastroschisis, two having compromised bowel perfusion at delivery and one having liver herniation. Cause of death was directly related to the gastroschisis in two infants; in one infant cause of death was recorded as hypoxic ischaemic encephalopathy. Death occurred on days 1, 2 and 10.
Discharge information was completed for 111 infants (86%). Average time to discharge home was 49 days (range = 13-262 days). This was on average 49 days in the silo group (range = 13-262 days) compared with 45 days (range = 14-212 days) in the primary repair group.
Conclusion
Gastroschisis is the most common anterior abdominal wall defect. Management includes either primary closure or staged reduction using a silo. There has been a trend towards using preformed silos over recent years. The majority of these infants have a good outcome without complications. Our experience supports the finding that infants with a diagnosis of complex gastroschisis have an increased risk of mortality. This review provides useful information on the management and outcome of babies with gastroschisis, which can be used in parental counselling.
Dedication
Dr Shree Vishna Rasiah

Management and outcome for babies born with a gastroschisis is dedicated to the memory of our dear friend and colleague, Dr Shree Vishna Rasiah, lost to COVID-19 in April 2020. Vish worked as a consultant neonatologist and cardiology lead at Birmingham Women’s Hospital. He was also the lead for the South West Midlands Newborn Network. He was an incredibly gifted doctor and a kind and compassionate healer. He saved the lives of countless newborn babies and helped improve the experience of families, by helping to streamline patient pathways and supporting them through their difficult journey.
Vish was a passionate teacher. He inspired and supported junior doctors, ANNPs, nurses and AHPs to undertake audits and research projects, encouraging them to present and publish their work. He patiently taught many doctors how to perform echocardiograms, instructed on ECHO and NLS courses, and collaborated with paediatric cardiologists to improve the pathways for babies with congenital heart disease. He was determined to improve neonatal outcomes through joint learning from mortality reviews.
He captured the joys of joint working and team bonding through his camera lens and shared it in social media. He celebrated life and encouraged all to join in the celebration whether it was with parents, staff and charities on World Prematurity Day, staff having Christmas celebrations, weekly cake Thursdays, team socials at the bowling alley, rock climbing or Bollywood night. He supported the Libby Mae Angels charity and guided them to get equipment for neonatal units across the West Midlands.
Vish’s actions inspired others to dream and do more. His legacy now lives through the people he trained.
Sarah Louise Williamson, Louise Lawrence, G. Suren Arul
Or read this article in our
Tablet/iPad edition
- The survival of gastroschisis in high income countries is now greater than 95%.
- Complex gastroschisis has worse outcomes than simple gastroschisis.
- Surgical management aims to reduce the herniated viscera and close the abdominal wall defect. This can be achieved by primary closure or staged reduction.
