

Exposure to noise during neonatal transport and its impact on hearing
Very low birth weight infants and neonatal intensive care unit survivors have a well-recognised increased risk of hearing loss. Neonatal units and especially neonatal transportation are acknowledged as sources of excessive noise. Although noise is well recognised as a cause of hearing loss in adults, there is paucity of data in neonates. In this study we measure the noise level exposure to babies during inter-hospital transfer and assess any associated hearing loss over this period.
Tayyaba Yasmeen
ST5 Paediatrics
Neonatal Transport, Scottish Ambulance Service
tayyabayasmeen@nhs.net
David Young
Senior Lecturer, Department of Mathematics and Statistics, University of Strathclyde, Glasgow
Alex Cheyne
Audiologist (retired), Biosense Medical
(now Interacoustics UK)
Stewart Guthrie
Consultant Neonatologist
Scottish Neonatal Transport Service (West)
stewartguthrie@nhs.net
Background
Babies born with very low birth weight and babies who require neonatal intensive care are at significant risk of hearing loss.1,2 There are many risk factors for acquired hearing loss in this population including aminoglycosides, loop diuretics, hyperbilirubinaemia, viral and bacterial infection, and hypoxia.1,3 It is well recognised that noise exposure is a cause of hearing loss or impairment in adults.4 Noise is known to stress babies and, despite our best efforts, noise levels thought excessive are encountered in neonatal intensive care units (NICUs) and on neonatal transport. What is not known is whether these noise levels cause hearing loss in babies, particularly given they are already unwell.5
When sound waves reach the ear they are transmitted through the outer ear to the ear drum (tympanic membrane) which moves the small bones (ossicles) of the ear, which in turn transmits to the fluid-filled cochlea. The cochlea contains many hair cells, which when moved generate electrical signals. These electrical signals are transmitted to the brain, which interprets them into the sensation of sound.1 Excessive noise levels can flatten the hair cells of the cochlea resulting in transient hearing impairment. If excessive noise exposure is recurrent or extreme then hearing impairment can be permanent and profound.4
There are many methods for assessing hearing acuity in adults. Pure tone audiometry is considered the gold standard. In pure tone audiometry patients respond by pressing a button when sequential tones of a given frequency and volume are played. This produces an accurate graph of the ability of the person to hear different frequencies and how loud they need to be played before they are heard.4 Unfortunately this method cannot be used with babies or indeed anyone who is unable to manually respond when needed. There are many automated tests available to use in babies, the most commonly used being ABR (auditory brainwave response) and OAE (oto-acoustic emissions) used in hearing screening programme6 A version of the OAE test called DPOAE (distortion product oto-acoustic emission) is generally considered the best for assessing noise-induced changes in the cochlea of the ear.7 In a healthy ear, any sound transmitted echoes back from the cochlea and back out of the ear; this sound is the OAE. We cannot hear these OAEs but they can be measured using very sensitive microphones. Hearing tests are normally performed in as quiet conditions as possible to improve test sensitivity. Ex-preterm babies usually have hearing tests performed close to discharge when they are well grown and in good health. It is unknown whether hearing tests, and in particular DPOAEs, can accurately be performed in busy NICU environments, in sick babies needing intensive support.
In Scotland all inter-hospital neonatal transfers are performed by a dedicated team of midwives, ANNPs and doctors. Approximately 700 transfers are performed in the west of Scotland annually via ambulances, helicopters and aeroplanes. Staff frequently complained of transient hearing impairment post-transfer and now have hearing protection provided and annual hearing surveillance performed by the Occupational Health Department. There was concern that this noise could be damaging the babies’ hearing. This study was performed to assess whether inter-hospital noise exposure could be a cause of hearing loss in babies. This was investigated in four ways;
- A pilot study testing the feasibility of DPOAEs in the NICU, high dependency unit (HDU) and special care baby unit (SCBU) neonatal inpatients.
- Performing DPOAE hearing tests before and after inter-hospital transfer then assessing any difference.
- Measuring the noise exposure of these same babies during transfer.
- Performing a frequency analysis of the noise on transfer.
Methodology and results
The study objective was to measure the noise level exposure to babies during inter-hospital transfer and assess any associated hearing loss over the transfer period. The study involved babies transferred by the West of Scotland Neonatal Transport team over a period of 18 months. A pilot study was performed assessing the viability of DPOAE hearing tests in babies of various sizes and sickness levels. Guided by the pilot, noise exposure and impact on hearing were further studied.
1. A pilot study testing the feasibility of DPOAEs in neonatal inpatients
This pilot study was performed to assess whether DPOAEs could be performed in small, preterm and sick neonatal unit inpatients. It was performed in the level 3 neonatal unit of the Princess Royal Maternity Hospital in Glasgow, Scotland. Babies of a full cross section of birth weights, gestations, postnatal age, ventil-atory support, dependency category and location within the neonatal unit were identified, consented and tested. DPOAEs were performed using the Scout Otoacoustic Emissions System 3.45.00. A range of frequency protocols were tested for feasibility. It was aimed to test up to 20 babies in this pilot stage. The exclusion criteria were known ear anatomical abnormality and not passing universal hearing screening.
Results
In the pilot stage we tested DPOAEs on 17 babies in total who were in SCBU, HDU and ICU categories. DPOAEs were successfully measured in babies as light as 730g and as young as a corrected gestational age of 29+5 weeks. We demonstrated DPOAEs in self-ventilating babies and in an invasively ventilated baby. We were unable to perform DPOAEs while on nasal continuous positive airway pressure (nCPAP; two babies tested) due to too high background noise despite using the ‘high noise’ setting on the machine.
2. Performing DPOAEs before and after inter-hospital transfer
Guided by the pilot study, appropriate babies transferred by the west of Scotland regional neonatal transport team had DPOAEs performed immediately (within 10 minutes) before and after the transfer. In this way the babies would act as their own controls cancelling out the effect of other variables. Haemoglobin level, gentamicin, vancomycin, furosemide and inotrope use, as well as a recent blood gas if relevant were recorded to inform of possible synergy if hearing loss was to be found. The DPOAE results were then interpreted by an experienced audiologist to identify a clinically significant change. The audiologist was blinded to the charac-teristics and noise exposure of the babies.
Results
Twenty-three babies were transferred and had DPOAEs tested before and after transfer. Four babies failed to demonstrate a DPOAE before the transfer. This could be for many reasons, for example fluid in the ear canal. One further baby failed a test as a result of the probe coming out of the ear during the test. This left 18 babies who successfully had DPOAEs produced before and after transfer.
No clinical difference was seen between the DPOAE hearing tests before and after transfer in any of the babies tested. In other words, no hearing loss was demonstrated in any of the babies transferred.
None of the babies transferred required a new intervention during transfer or had a clinically apparent deterioration. No oto-toxic medications were given during transfer.
All of these transfers were performed, at least in part, by road using one of the dedicated neonatal transport ambulances. Three transfers were performed by air; one using military helicopter to a Hebridean island and two using a Scottish Ambulance Service’s Beach King Air aeroplane to England and Wales where a local A&E ambulance was used to complete the transfer. In two transfers the siren was used. Three transfers used car seats, 17 used incubators. The median transfer duration was 1hr 3min, (range 31min to 3hr 53 min).
The babies tested ranged from a corrected gestational age of 30+0 to three weeks post-term, from day 1 to day 75 post-birth. Seventeen babies were self-ventilating in air, three were in nasal oxygen up to 0.5L/min and three were invasively ventilated.
Three transfers were to the tertiary children’s hospital for an MRI scan then back to the referring unit. The noise exposure of these scans could not be measured as the noise level meters are metallic so could not be taken into the scanner.
3. Measuring the noise exposure of these same babies during transfer
The same transfers had the noise exposures measured by Cirrus CR:110A doseBadge Personal Noise Dosimeters. One dosimeter was placed on the outside of the incubator and one on the inside to allow calculation of the noise level change caused by the incubator. If travelling in a car seat then only one dosimeter was used. These noise level meters underwent two-point calibration before each use. The dosimeters were securely placed such as to prevent artefact interference and patient harm. When placed inside the incubator they were placed as near as practically possible to the subject’s ear.
Results
Twenty babies were tested on transfer for noise exposure; three fewer than were tested for DPOAE change. This was because three pairs of twins were transferred and in each case both twins had DPOAEs tested but only one could have the noise exposure tested due to the availability of only two noise level meters (one inside and one outside the incubator per baby). Furthermore three babies were transferred not in incubators but in car seats. From 23 babies transferred this gave noise exposure data on 17 babies in incubators and three in car seats. In the incubator group the noise levels inside and outside were compared. In the car seat group the data obviously could not be compared in this way but is given simply to show noise exposure. In each group the noise exposure data is given in two ways. Firstly, the average noise exposure during the measured time period, ‘Leq’. Secondly, the highest noise level recorded at any point during the measurement, ‘Peak’.
- The Incubator (inside): Leq median 72.5dB (range 69.8-80.0); peak 123.30dB (range 126.9-133.2)
- Car seat: Leq median 79.4dB (range 78.2-79.6); peak 131.8dB (range 127-137.2)
Data were statistically analysed using the Wilcoxon signed-rank test (Table 1 and figure 1).
In the small number of babies transferred by car seat (three); these babies had median noise exposures (Leq) 6.9 decibels louder (median 79.4dB, mean 79.2dB, range 78.2-79.6dB) and median peak levels 4.9 decibels louder (median 131.8dB, mean 132dB, range 127-137.2dB) compared with inside the incubator. The small numbers in this car seat group makes meaningful statistical comparison impossible. Data are given for interest and to show the noise exposure relating to these hearing tests (DPOAE) results.
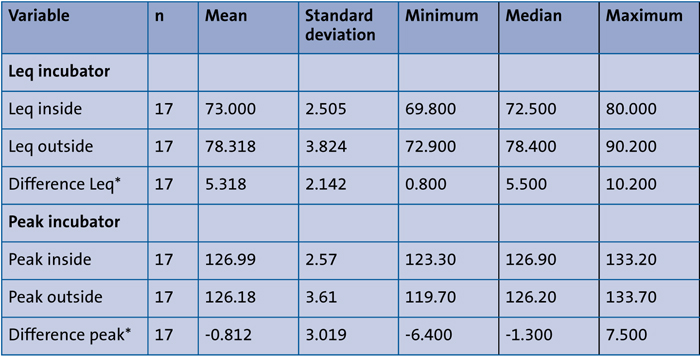
TABLE 1 The average (Leq) and highest (peak) noise exposures inside and outside the incubator using the noise dosimeters. *The minimum and maximum numbers are the highest and lowest numbers in the study; not necessarily from the same baby. The differences relate to the smallest, largest and median differences between inside and outside on each individual baby (therefore the numbers are not directly calculable from the table).
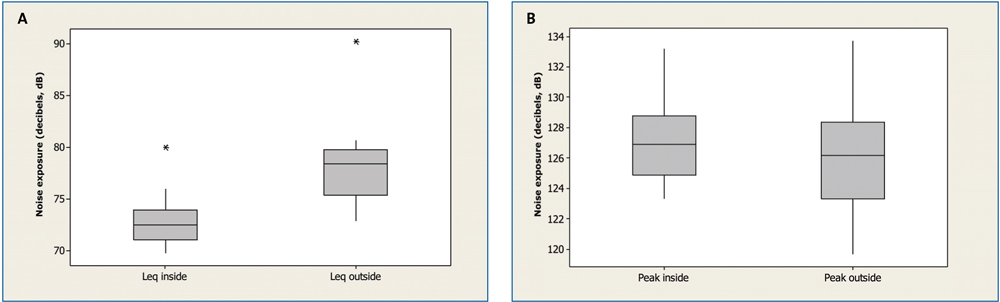
FIGURE 1 Boxplots. A) Average noise exposure (Leq) inside and outside the incubator during transfer. The Leq outside was significantly higher than inside p<0.001. The median difference was 5.5dB with approximate 95% CI (4.2, 6.2). This is a clinically significant difference. B) Median peak noise exposure inside and outside the incubator during transfer. There was no evidence of a statistically significant difference in the median peak inside and outside p=0.142.
4. Performing a frequency analysis of the noise on transfer.
The noise level meters measured average and peak noise level. The frequency of the noise produced on transfer was measured by a Brüel & Kjær model 2230 precision sound level meter, IEC type I instrument. A frequency analysis of the noise levels inside and outside the incubators was measured three times while travelling at average speed and conditions. This was measured in the neonatal transport ambulance when travelling without the patient on-board. This sound level meter is significantly larger than the personal noise dosimeters and could not safely be secured. As such no baby was in, nor could be in, the incubator at the time of measurement.
Results
Measurements were taken on three separate occasions and measurements taken from 31.5Hz to 16kHz. They were taken in the road ambulance while driving at a steady and average speed while en-route to pick up a baby. As such the conditions were as close as possible to the noise levels a baby would experience without actually having the baby on board. As previously mentioned, the frequency analysis could not be performed safely with the baby in the incubator while moving due to the size and weight of the frequency sound level meter. The noise level results were statistically tested using a general linear model to analyse noise levels in relation to frequency and location.
A general linear model was used to analyse noise levels in relation to frequency and location. There was a significant difference between the frequencies (p<0.001) and between the locations (ie inside and outside, p<0.001). The inter-action between location and frequency was significant, p<0.001. This is illustrated in figure 2.
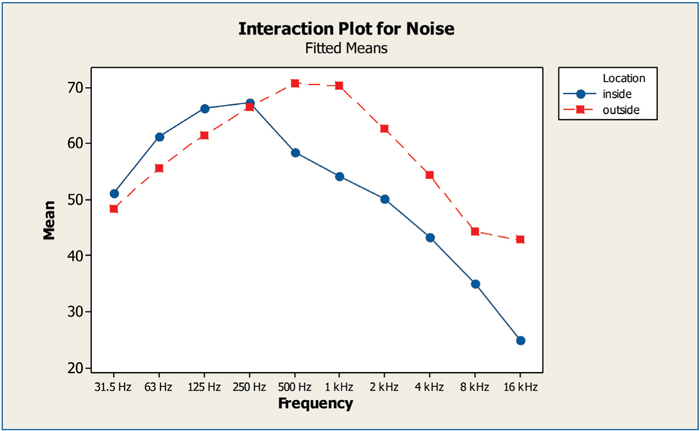
FIGURE 2 Relationship of noise levels with frequency and location (inside vs outside the incubator) statistically analysed by general linear model. This shows the incubator is selectively protective at mid to high frequency sound and not at low frequency sound. The reduction is as much as 17.9dB at 16kHz.
Discussion
It is reassuring that these transfers did not result in identifiable hearing loss to this already fragile population. This cannot be taken to imply that no noise-induced hearing loss can occur in this population, particularly chronic noise exposure. Nor can it imply that noise reduction measures are not required. Noise levels are known to stress babies making noise reduction an important NICU goal.1,2 These transfers are significantly noisy when compared to suggested noise limits and UK workplace limits.8
Incubators are protective to average sound levels but not to peak sound levels. This may suggest some of the source of the peak noise originates within the incubators. Fastidious care needs to be given to ensure no rattling or contact of equipment can occur inside the incubator. Incubators selectively protect mid to high frequency noise. This is particularly helpful as high frequency noise is known to be most harmful to hearing.4 This also implies that babies transferred not in an incubator are exposed to higher noise levels. This was shown in the small number of babies transferred by car seat. This has implications for the use of car seats by transfer teams. The west of Scotland neonatal transport service no longer uses car seats to transfer babies.
This is a small study designed to assess the safety of noise exposure on transfer to babies’ hearing. We measured immediate damage to the hair cells following noise exposure during transfer and it is therefore not possible to comment on long-term/later damage. In order to ensure that we did not get false positive results in babies who might have already suffered some damage to the hair cells due to noise exposure in the NICU, congenital hearing loss or other reasons (eg gentamicin, hyperbilirubinaemia, etc), we performed baseline pre-transfer DPOAE assessments. This study was not designed to be a definitive study of the thresholds of noise-induced hearing loss in babies. It is clearly unethical to expose babies to varying levels of noise to assess noise exposure hearing loss thresholds. The noise exposure to babies on transfer is already limited as much as practically possible, but there remained concern that transfers were causing harm. The strengths of this study are:
- It tests a common noise exposure, which is likely to be the highest short-term noise exposure neonatal unit inpatients are exposed to.
- Babies act as their own controls during the study, as other than noise there were no other significant compounding effects during the transfer period.
As mentioned, three of the transfers were for an MRI scan and the noise exposure of this could not be measured. However despite this extra noise exposure there was no hearing loss identified.
Having identified high noise levels we were concerned about staff exposure given the frequency dedicated transport team staff perform transfers. A separate study was performed assessing staff noise exposure resulting in the provision of hearing protection.9 Our ambulances are reviewed to reduce noise to a minimum. We would encourage all transport networks to consider noise when purchasing or reviewing transport vehicles and equipment.
Conclusion
It is reassuring that no hearing loss was demonstrated following the noise exposure of inter-hospital transfer, but this does not mean noise reduction is not required or chronic noise exposure is not of concern. Incubators reduce the noise exposure of neonates, although the noise level is still significantly higher than the UK workplace noise limits. Noise levels need careful consideration when procuring and using ambulances and medical equipment. Further studies to assess noise levels with different types of respiratory support as well as ways to reduce noise exposure to newborn infants are required.
Approvals and consent
This study was performed with the approval of the local research ethics committee and the research and development office. Written, informed parental consent was obtained for all parts of this study.
Acknowledgements
The authors are grateful for the input and kind help of Lesley Jackson, Suzie Wills, Elaine Foye and Kate Campbell. This study was funded by a grant from Defeating Deafness UK. The DPOAE machine was given free of charge by Biosense Medical (now Interacoustics UK) as was their expertise. The Brüel & Kjær model 2230 precision sound level meter was donated for the study by Strathclyde University.
Or read this article in our
Tablet/iPad edition
- Noise exposure and impact on hearing was assessed in babies transferred by the West of Scotland Neonatal Transport team over a period of 18 months.
- No hearing loss was demonstrated following inter-hospital transfer; however, noise reduction is still required and chronic noise exposure is still of concern.
Also published in Infant:
