

Antenatal optimisation for preterm infants less than 34 weeks: a quality improvement toolkit
The British Association of Perinatal Medicine (BAPM) and the National Neonatal Audit Programme (NNAP) are collaborating on four quality improvement toolkits to support perinatal staff to implement the evidence around perinatal optimisation. This article presents the Antenatal Optimisation Toolkit. The evidence for key interventions is described alongside a quality improvement journey, which supports staff to choose improvement solutions most suitable for the local context.
Lauren Shaw
Neonatal Grid Trainee, East Deanery, Scotland
Julie-Clare Becher
Lead for Quality, BAPM and Consultant Neonatologist, Royal Infirmary of Edinburgh,
julie-clare.becher@nhslothian.scot.nhs.uk
On behalf of the BAPM Antenatal Optimisation Toolkit Group
Prematurity is the most significant cause of mortality in children under five and is associated with significant morbidity in surviving infants. Many well-established evidence-based antenatal interventions reduce the risk of neonatal death and associated preterm morbidities but UK audit data show there is variable uptake in these interventions with wide variability between units and networks.1 BAPM aims to improve standards of perinatal care by optimising the skills and knowledge of all those involved in providing this care. A key value of BAPM is ‘working collaboratively’ to provide the safest and most effective service for babies and families by delivering high quality perinatal care and provide support for perinatal professionals.
NNAP2 is commissioned by the Healthcare Quality Improvement Partnership (HQIP), delivered by the Royal College of Paediatrics and Child Health (RCPCH) and funded by NHS England along with the Scottish and Welsh Governments. The NNAP assesses whether babies admitted to neonatal units in the UK receive consistent high-quality care. It sets evidence-based standards on key clinical outcomes and in turn identifies areas for quality improvement (QI) concerning the delivery and outcomes of neonatal care.
With these shared goals in mind, BAPM, NNAP and other key stakeholder organisations in perinatal care are collaborating in a three-year national QI initiative that will target key NNAP measures. This initiative will align with and support other neonatal national quality workstreams such as the Maternity and Neonatal Safety Improvement Programme (MatNeoSIP)3 in England, and the Maternity and Children Quality Improvement Collaborative-Scottish Patient Safety Programme (MCQIC-SPSP)4 in Scotland. The work is aligned with the Saving Babies’ Lives Care Bundle (SBLCBv2).5 Each improvement drive includes a QI toolkit mapped to the BAPM Neonatal Services Quality Indicators (NSQI)6 and has been developed by clinicians who have demonstrated excellence in the area of focus, led by the multi-disciplinary BAPM Quality Steering Group.
The toolkits have been designed using well-established QI methodology and under the RCPCH Quality Improvement in Child Health Strategic Framework.7 The toolkits introduce essential QI tools and methods that are quick to learn and easy to apply and can be used as a practical step-by-step guide to improvement. In addition, the BAPM website also offers a range of free QI resources, links to easy-to-use templates and e-learning, QI tutorials and a forum for shared learning (www.bapm.org/quality).
Context for the toolkit: the Perinatal Optimisation Care Pathway
Perinatal optimisation refers to the process of reliably delivering evidence-based interventions in the antenatal, intrapartum and neonatal period to improve preterm outcomes. Examples of current perinatal optimisation initiatives, which aim to result in the consistent application of a bundle of interventions, are those of the West of England Academic Health Sciences Network PERIPrem bundle8 and the SPSP-MCQIC Preterm Perinatal Wellbeing Package.9 The BAPM Perinatal Optimisation Care Pathway (FIGURE 1) refers to these various interventions as they occur over time applying to both the mother and her preterm baby and aligns with key elements of the aforementioned initiatives. The pathway is supported by four BAPM toolkits (Antenatal Optimisation, Optimal Cord Management, Normothermia10 and Maternal Breast Milk). Additional perinatal optimisation interventions such as respiratory management are acknowledged but are not yet included in this pathway.
The Perinatal Optimisation Care Pathway sits within the remit of the local and network ‘perinatal team’ whose strong team-working culture, high quality communication habits and pursuit of common goals result in the reliable delivery of these protective interventions. Such implementation success can only occur within a favourable ‘quality context’ where the structure and processes support an optimal environment for delivering QI. Such key contextual features are described in the BAPM Neonatal Service Quality Indicators.6 Throughout the pathway, high quality communication about risks and benefits of interventions should take place with parents. In the context of extreme preterm gestations, the principles of the BAPM Extreme Preterm Framework should be adhered to, including a joint discussion between the parents and both a senior obstetrician and neonatologist, and which includes a risk-based assessment of prognosis.11
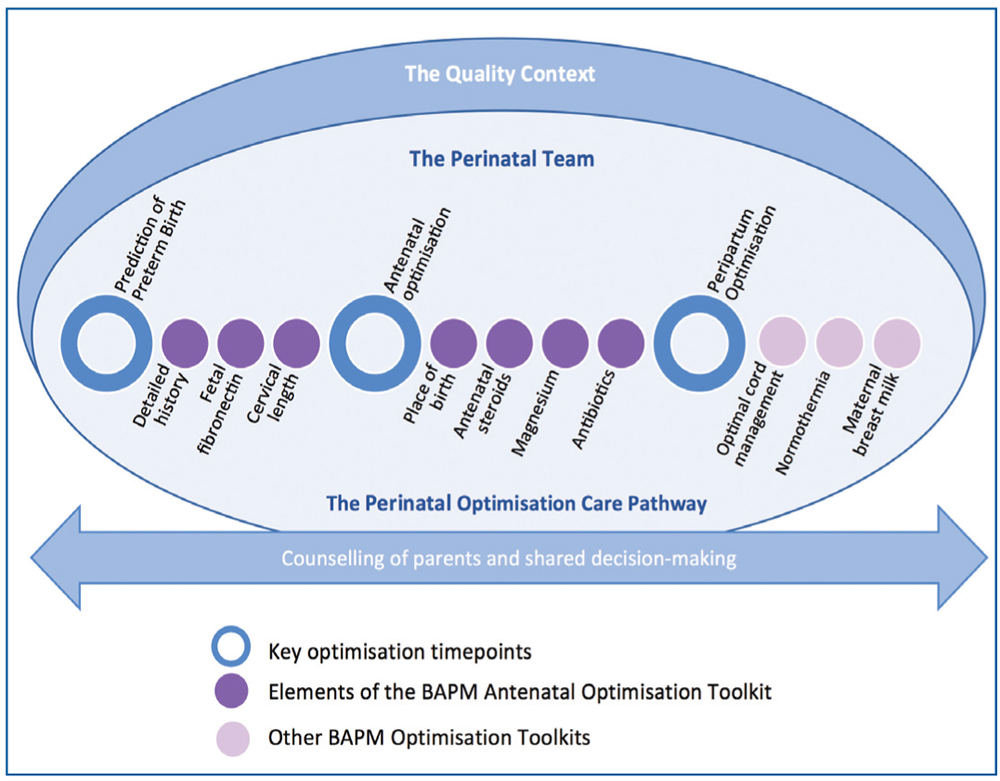
FIGURE 1 The Perinatal Optimisation Care Pathway.
How will a QI toolkit help me implement antenatal optimisation?
The Antenatal Optimisation Toolkit provides:
- the rationale for antenatal optimisation QI when you and your team, or those supporting the project at executive level, require to know the evidence for change
- easy to use QI tools to understand where you are now and what you need to commence your project without any prior QI experience
- guidance about how to build your team and secure buy-in for your project
- examples of QI that have been shown to be successful in improving antenatal optimisation for very preterm babies, including improvement stories from high performing units
- tools to help you measure and understand the impact of your changes
- examples of how to embed change and sustain momentum including parent experience stories.
Key elements of the toolkit
The key elements of antenatal optimisation and their rationale can be seen in FIGURES 2 AND 3.
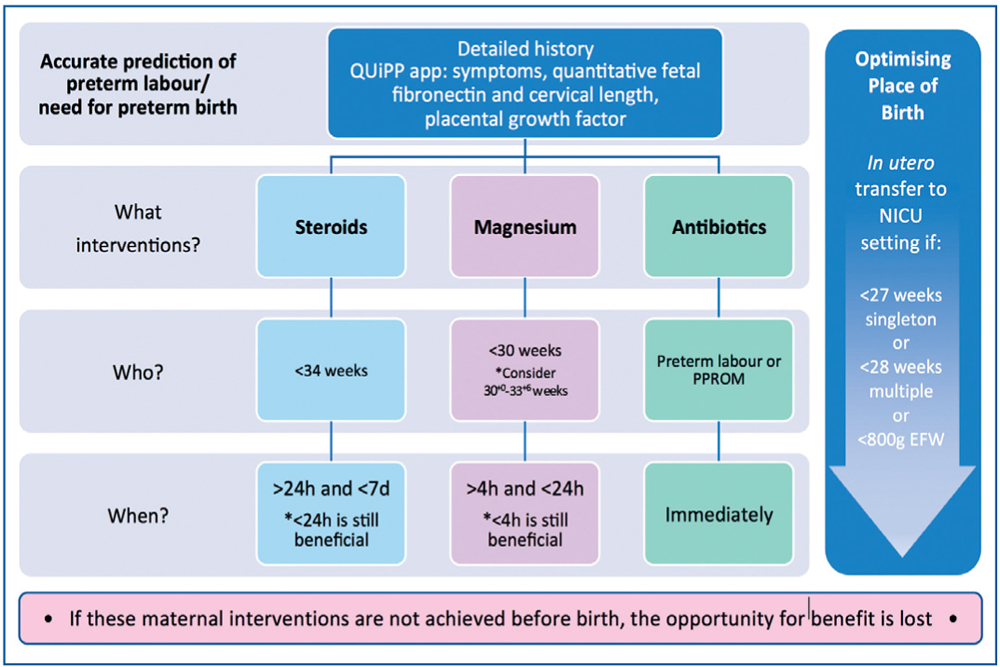
FIGURE 2 Key elements of the antenatal optimisation care bundle. Abbreviations: QUiPP app=clinical decision-making tool for preterm birth prediction; PPROM=preterm pre-labour rupture of membranes; EFW=estimated fetal weight.
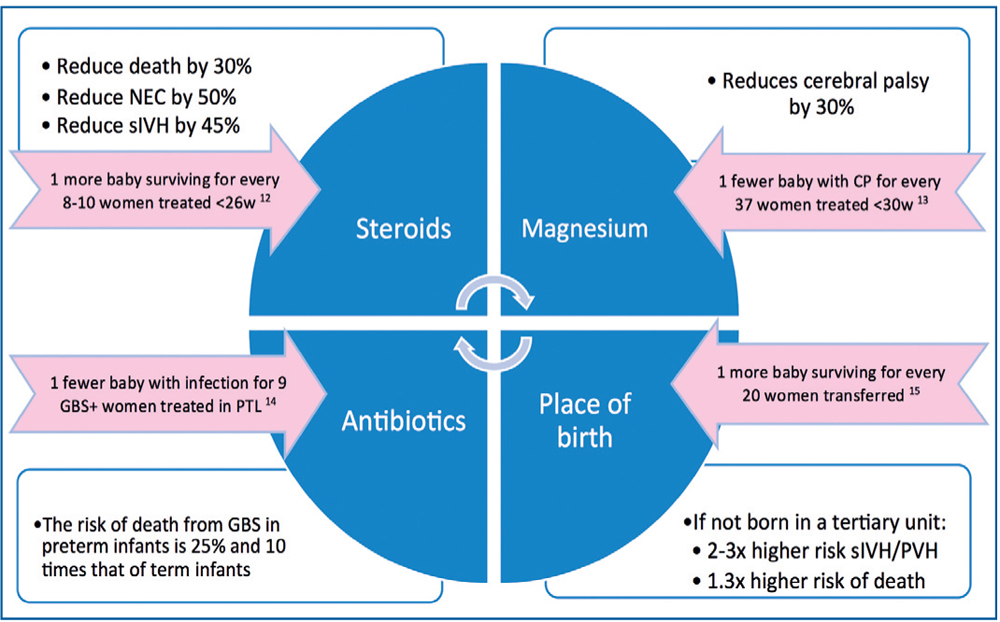
FIGURE 3 The rationale for antenatal optimisation to improve preterm outcomes.12-15 Abbreviations: NEC=necrotising enterocolitis; sIVH=severe intraventricular haemorrhage; CP=cerebral palsy; GBS=group B streptococcus; PTL=preterm labour; PVH=periventricular haemorrhage.
How should the toolkit be used?
This toolkit is a practical resource from which units who wish to improve compliance rates of antenatal optimisation measures can select the most suitable interventions for their particular context. In this respect it is not to be regarded as a guideline. For example, there are units which achieve high NNAP compliance with antenatal steroid administration but this may be at the expense of optimal timing, occurring more than a week before birth with many more women treated than those who go on to have a preterm birth. Another unit may have a lower compliance rate but the timing of administration is optimal. The improvement solution for each unit may be different. Similarly, optimal place of birth may be variably dictated by accuracy in predicting preterm birth or by referral, capacity or transfer issues. Individual units are encouraged to interrogate their processes in order to understand where and how optimisation measures are applied in their local setting and select interventions that are best suited to their context.
A useful mnemonic that summarises the elements and additional considerations raised by this toolkit can be seen in FIGURE 4.
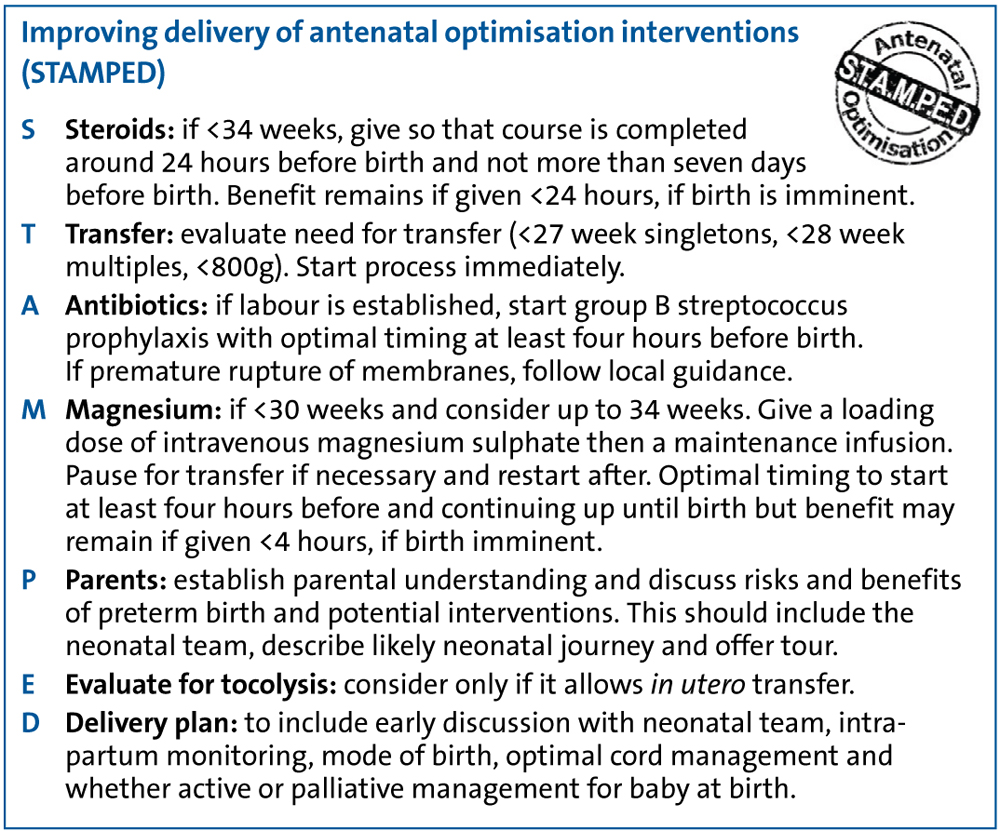
FIGURE 4 STAMPED: a useful mnemonic that summarises the key elements of the toolkit.
Where should we start?
Beginning any QI work can be a daunting task, particularly if it crosses multiple departments and specialties. In order to accomplish change it is essential to have a structured and well-defined process, as set out in this toolkit. We describe five phases of an improvement journey from defining the problem within your own local context, developing a shared purpose withinyour unit and team, to planning, implementing and testing and measuring, and finally ensuring change is embedded and sustained.
Phase 1: Defining the problem
Where are we now and how did we get here?
It is important to understand your local data, and to benchmark where possible in the context of regional, national and inter-national standards observing any changes over recent years. To achieve this your team should understand how to look at your local data, what questions to ask and where to access bench-marking data such as BadgerNet national reports and comparison charts, the network data dashboards, NNAP Online and Nightingale, Vermont Oxford Network. Finally, being able to convey these data to the wider team clearly and concisely will facilitate a stronger commitment to the implementation of QI interventions. The toolkit provides a useful list of questions to help interrogate your own data and to highlight where your most important changes need to happen. Once you have identified areas for improvement there are many tools available to help your team understand why eligible women may not receive optimised antenatal care. Examples include Pareto charts, fishbone diagrams and forcefield analysis. Within the toolkit there are many worked examples (FIGURE 5) and links to BAPM’s QI Made Easy resources.
For example, the Pareto chart in FIGURE 5 shows that around 80% of causes can be explained by three factors: a delay in diagnosis at the local neonatal unit, a lack of cot capacity at the neonatal intensive care unit (NICU) and women presenting too late in established labour. This problem will therefore require local, network and community solutions to solve. It is often through these processes that change ideas and insights will be generated. Using one or more of these tools will identify potential areas for improvement and ideas for change. These ideas can be organised into a driver diagram giving your project clear purpose and direction (FIGURE 6).
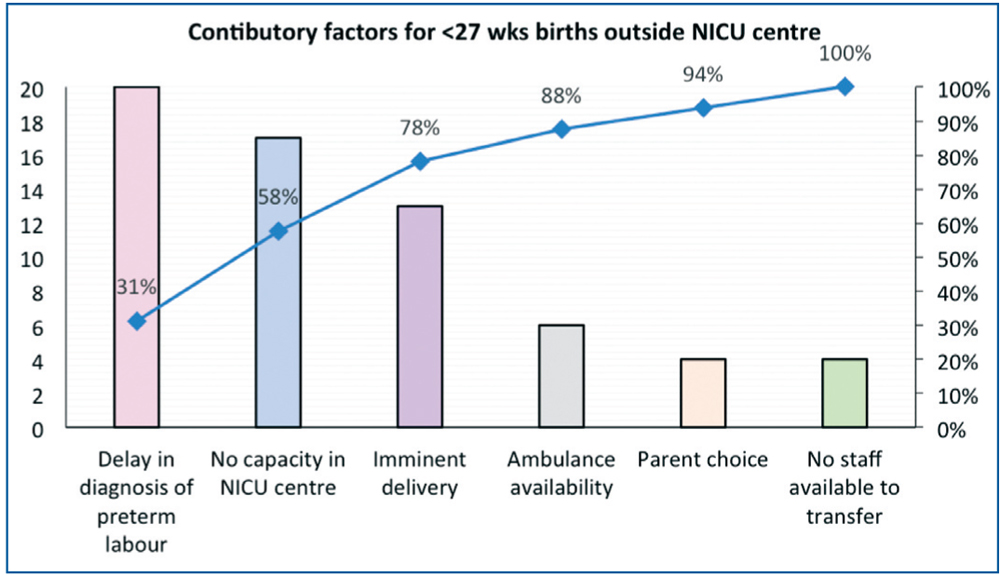
FIGURE 5 An example of a Pareto chart for place of birth. The chart shows that around 80% of causes can be explained by three factors: a delay in diagnosis, a lack of cot capacity at the NICU and women presenting too late in established labour.
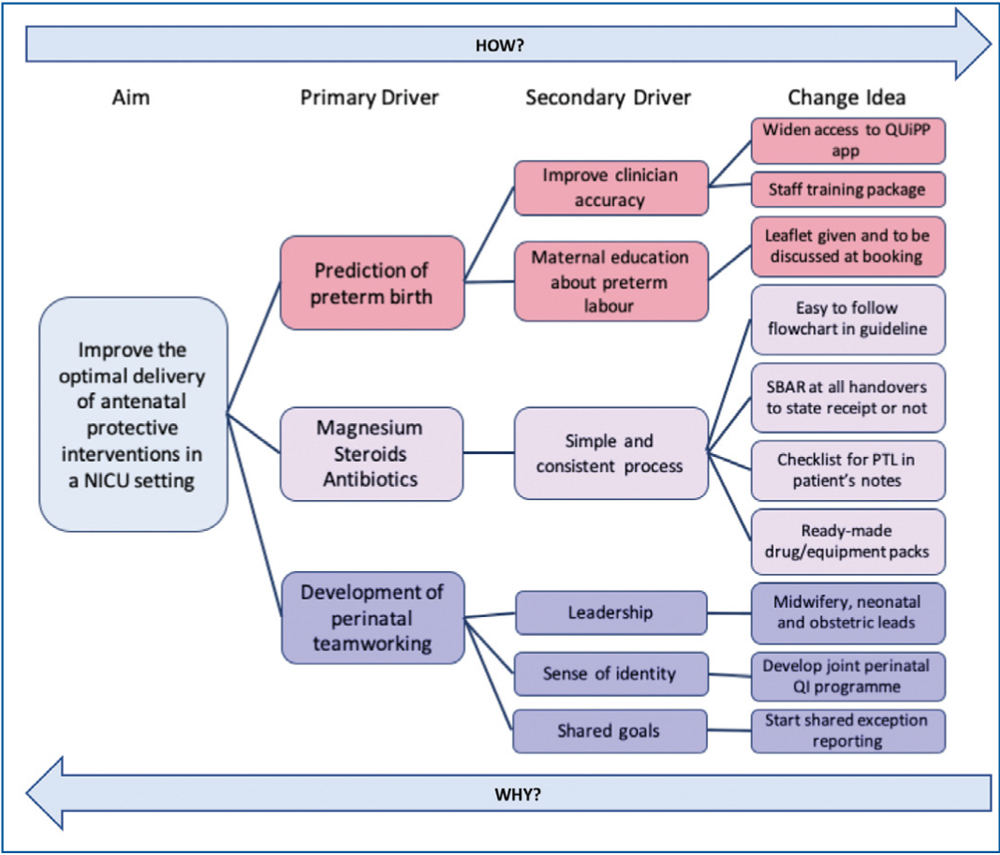
FIGURE 6 An example of a driver diagram to improve delivery of the antenatal optimisation pathway. Key: SBAR=situation, background, assessment, recommendation.
Phase 2: Developing a shared purpose
Who do we need in our team?
One of the key components to any successful project is having a team that is engaged, resilient, enthusiastic and committed to working together to create the right culture for change. Developing a strong perinatal team within your workplace will help facilitate communication, understanding and collaboration across departments and allow more cohesive implementation and imbedding of antenatal interventions. Having shared goals, a shared vision and sharing experience ensures your project has momentum and that barriers and enablers can be best appreciated and tackled. The toolkit highlights important questions to support you in identifying the right people to not only include in your team but other people impacted by or who can influence the magnitude of your improvement (stakeholders). In this it is vital to include the parental voice as their views give a different perspective and their stories form powerful tools for engagement and action. There are many such stories within the toolkit (FIGURE 7).
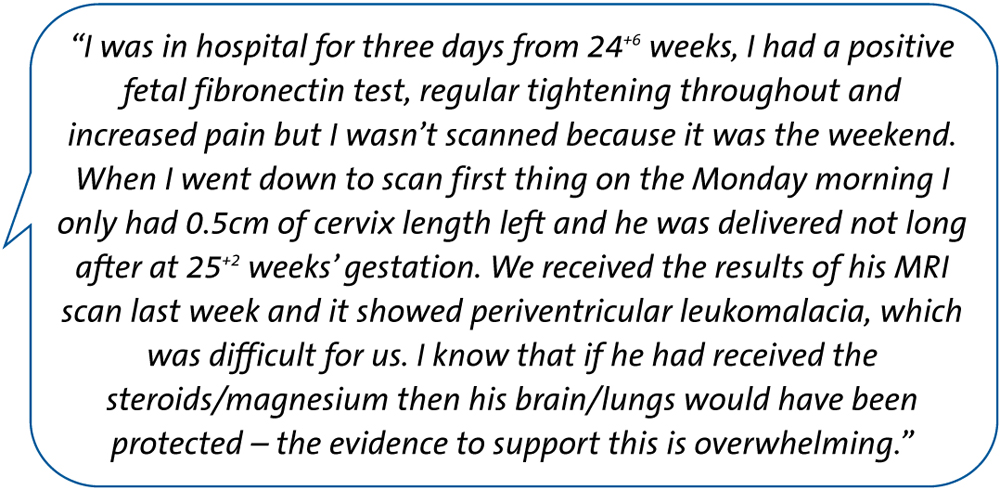
FIGURE 7 A parent’s story.
Phase 3: Plan and implement change
How do we test our change ideas?
There are a number of methodologies that can be adopted to implement a QI strategy but the one most widely recognised in health care is the Model for Improvement which encourages use of plan, do, study, act (PDSA) cycles (FIGURE 8). The toolkit describes how this approach can be used to help implement your change ideas for antenatal optimisation and signposts the BAPM online resources to support this process.
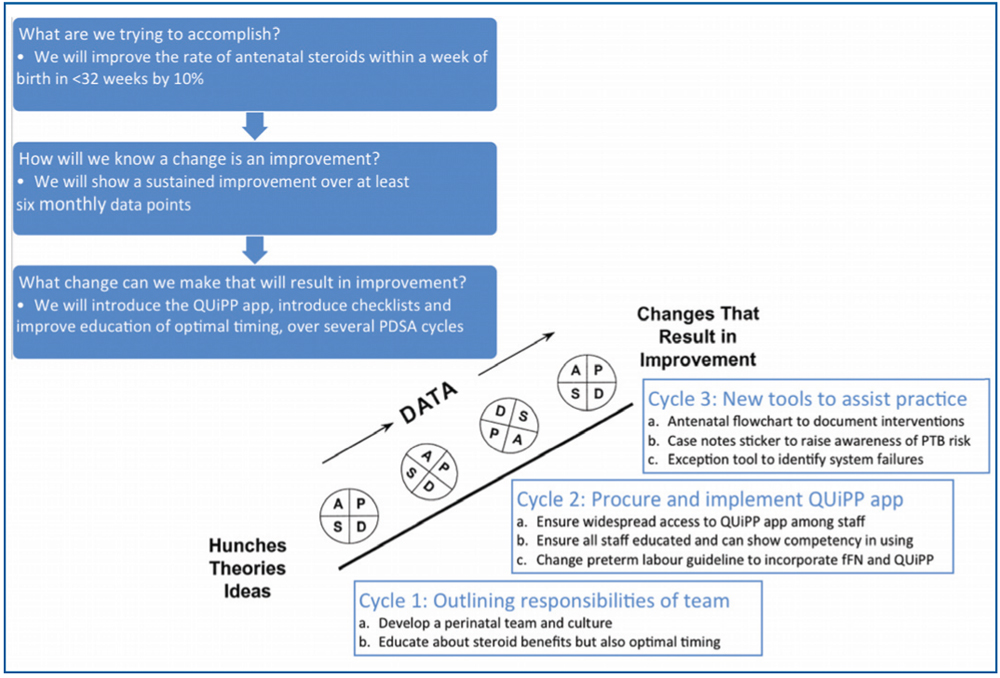
FIGURE 8 A PDSA schematic for antenatal optimisation. Abbreviations: PDSA=plan-do-study-act; PTB=preterm birth; fFN=fetal fibronectin.
Phase 4: Test and measure improvement
How do we know our change was an improvement?
Measurement of improvement should not be a ‘before and after’ audit, which is unreliable in measuring true change, but a continuous process over time during which your changes can be evaluated and modified. Within the toolkit there are examples of outcome, process and balancing measures as they relate to antenatal optimisation. Further consideration is given to how these data are displayed within your unit and includes examples that can be used by the QI team, such as run charts and statistical process control (SPC) charts, and more visual data sharing that is often easier to interpret for frontline staff and families.
Phase 5: Implement, embed and sustain
Our changes show improvement, how do we keep going?
Ensuring that change becomes embedded in routine practice throughout your system requires robust governance arrangements, such as adverse event and exception reporting and an early recognition of barriers and loss of motivation. It is not unusual to find the impact of a previous improvement lessens over time but it is important to understand why so that solutions can be tailored to the problem. There are many different approaches discussed within the toolkit, including re-examining your change idea, re-marketing your message (FIGURE 9), including using impactful stories or photos from families (FIGURE 10) and learning from high achieving units. There are also links to the highly useful NHS sustainability model.16
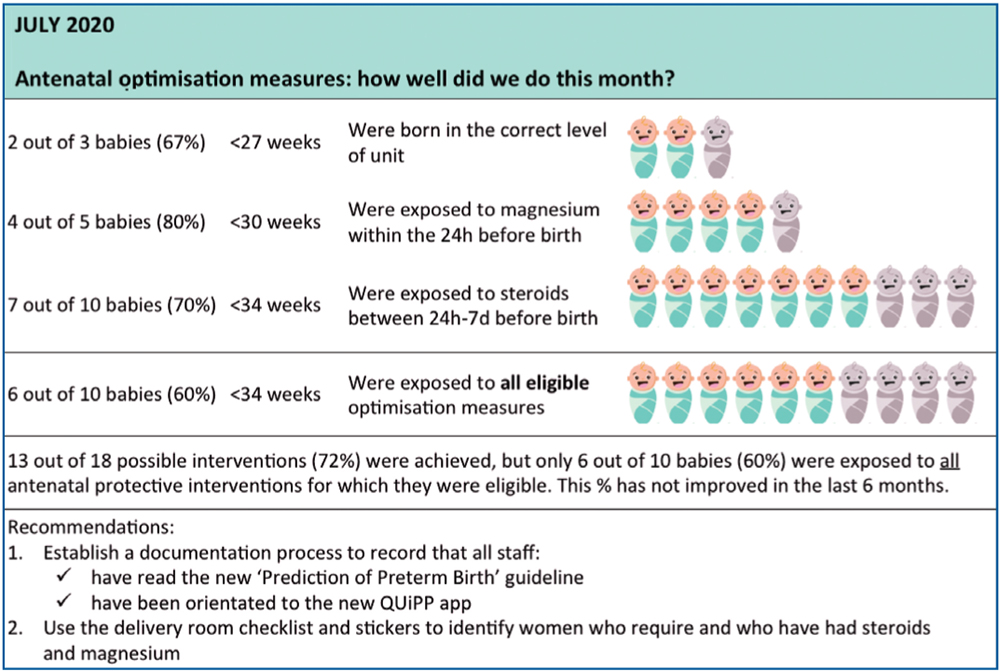
FIGURE 9 An educational poster to help engage staff in the importance of your project.
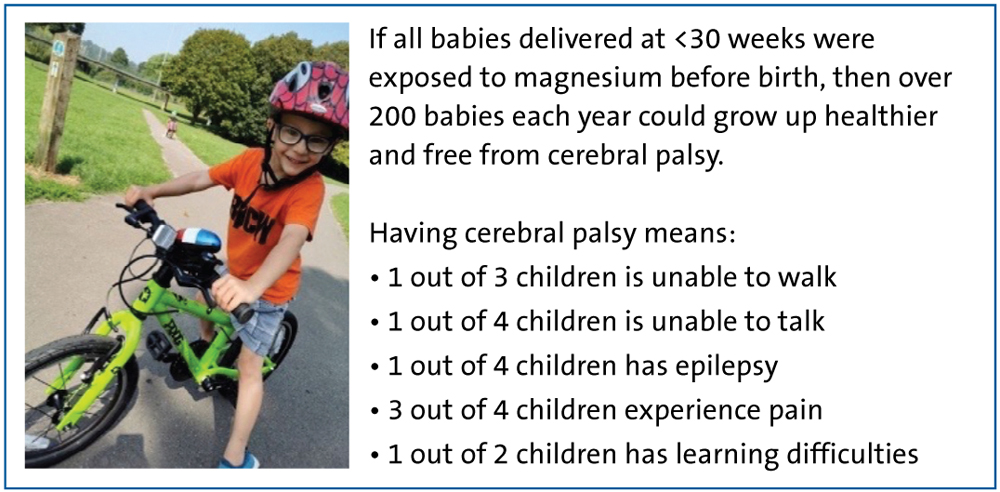
FIGURE 10 Using childhood outcomes to improve engagement.
Overall, this toolkit seeks to provide the wider perinatal team with a framework to help understand the local context for QI, the enablers and barriers to implementation, and gives a structured method to work through to ensure that key interventions can be more reliably delivered. It signposts an abundance of QI resources suitable for the uninitiated and the more experienced QI team and provides creative ideas for education and team engagement.
This toolkit was developed by a multidisciplinary team representing all areas of the perinatal pathway including midwives, neonatal nurses, obstetricians, neonatologists, national transport group and parent representatives. Last year BAPM released the Normothermia toolkit10 and we are excited about the upcoming launch of the Early Maternal Breast Milk and Optimal Cord Management Toolkits. We hope that this resource, together with the other toolkits, encourages you to foster a collaborative perinatal environment, working hand in hand with parents so that more preterm children in our care survive to lead happier and healthier lives.
Acknowledgements
The BAPM Antenatal Optimisation Toolkit Group: Debbie Bezalel, Bliss; Josie Anderson, Bliss; Manju Chandiramani, Guy’s & St Thomas’ NHS Trust; Cora Doherty, University Hospital of Wales; Cath Harrison, Leeds Teaching Hospital NHS Trust; Kelly Harvey, North West Neonatal Network; Vicky Hodgetts-Morton, University of Birmingham; Lawrence Impey, John Radcliffe Hospital; Tracey Kay, Royal Devon & Exeter NHS Trust; Karen Luyt, St Michael’s Hospital; Stephanie Michaelides, Royal College of Midwives Representative; Katie Morris, Birmingham Women’s NHS Trust; Sankara Narayanan, West Hertfordshire Hospitals NHS Trust; Elizabeth Osmond, St Michael’s Hospital; Colin Peters, Royal Hospital for Children, Glasgow; Ann Remmers, West of England Academic Health Sciences Network; Meekai To, Kings College Hospital London; Michele Upton, NHS Improvement; Alison Walker, Royal Maternity Hospital Belfast.
To find out more about the BAPM Antenatal Optimisation Toolkit visit: www.bapm.org/pages/194-antenatal-optimisation-toolkit
Or read this article in our
Tablet/iPad edition
