

COVID-19 surveillance swabbing in a tertiary NICU
Like other neonatal units around the world, COVID-19 raised many questions for us about personal protective equipment, parental presence, and how best to cohort babies in the neonatal intensive care unit (NICU). There is limited guidance on the use of routine swabbing to guide practice in neonatal care. However, as we were caring for a group of very vulnerable patients, it was felt that regular surveillance would provide the assurance to staff and parents that the unit remained safe and COVID-19 free.
Kristin Tanney1Consultant Neonatologist
kristin.tanney@mft.nhs.uk
Kath Eaton1
Lead Nurse, Newborn Services
Louise Hesketh2,3
Consultant Clinical Scientist in Virology
Ngozi Edi-Osagie1
Consultant Neonatologist
1. Newborn Intensive Care Unit, Manchester University NHS Foundation Trust
2. Clinical Virology, Manchester University NHS Foundation Trust
3. Public Health England
With the support of the Clinical Virology and Infection Prevention Control teams, we instituted twice weekly surveillance swabbing
for those babies who were deemed high-risk, ie all of our babies who were undergoing aerosol-generating procedures.
We audited the COVID-19 tests performed over a 10-week period between 1 May 2020 and 10 July 2020. Inborn babies were not routinely swabbed as expectant mothers in labour had rapid swabs taken in line with NHS England guidance1 for testing non-elective admissions. This meant that for the majority of cases, we were aware of maternal COVID-19 results before babies were admitted to the neonatal unit.
A total of 464 tests were undertaken. These were predominantly surveillance swabs (n=350) but also included swabs or secretions sent following external admission (n=23), swabs taken when inborn babies’ mothers’ status was unknown (n=55), pre-operative testing (n=6), swabs taken due to clinical deterioration (n=10) and reasons listed as ‘other’ (n=20).
Out of the 464 COVID-19 tests undertaken, we had three positive results, detailed in table 1.
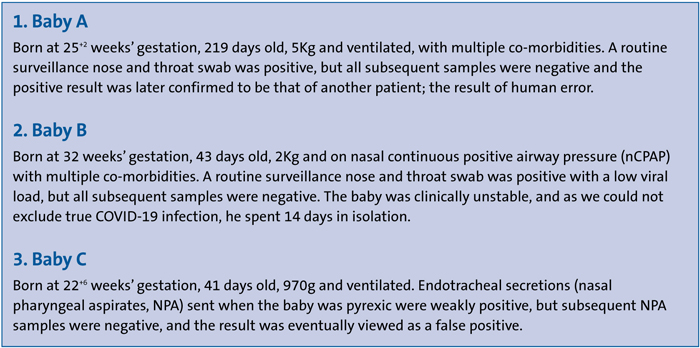
TABLE 1 Three out of 464 COVID-19 tests were positive.
With the benefit of hindsight, we understand a bit more about the relevance of sample size and type, and that PCR (polymerase chain reaction) testing does not always provide a black-or-white result. Results need to be interpreted in tandem with the clinical picture and progression, and actions should always lie on the side of suspicion when there is so much at stake.
With these babies, we took the cautious approach of isolating until multi-professional conclusion was reached, even though this caused some distress to their parents. We feel that our surveillance swabbing experience in the NICU during this global pandemic is quite unique, and we have gained much from the assurance that the almost-entirely negative findings have allowed.
For now, we continue once-weekly surveillance swabbing for COVID-19, using it to guide our practice during these unprecedented times.
Or read this article in our
Tablet/iPad edition
