

A neonatal nutrition network for sub-Saharan Africa
In 2018, seven neonatal units (NNUs) in Nigeria and Kenya collaborated with the Liverpool School of Tropical Medicine to establish NeoNuNet – a neonatal nutrition network in sub-Saharan Africa. By the sharing of expertise and experience, NeoNuNet hopes to improve clinical outcomes of preterm and low birthweight (LBW) infants across the region.
Macrine Adhiambo Olwala
MBChB, Medical Officer, Paediatric Department, Jaramogi Oginga Odinga Teaching and Referral Hospital (JOOTRH), Kisumu, Kenya
molwala@gmail.com
Walter Otieno
MBChB, M.Med (Paediatrics), PhD, Senior Lecturer and Head of Department of Paediatrics and Child Health, Maseno University School of Medicine and Consultant Pediatrician at JOOTRH
walter.otieno@usamru-k.org
Grace M. Nalwa
MBChB, M.Med (Paediatrics), Lecturer in Paediatrics and Child Health, Maseno University School of Medicine and Consultant Paediatrician at JOOTRH
gracemjnalwa@gmail.com
In 2014, approximately 10.6% of all live births globally were born preterm.1 This translates to 15 million babies born preterm annually. Prematurity is the single most important cause of death in the neonatal period and is the second-leading cause of death in children under five years.2 This morbidity and mortality burden is higher in lower- and middle-income countries (LMICs), with South Asia and sub-Saharan Africa accounting for almost two-thirds of the world’s preterm babies, and over three-quarters of the world’s newborn deaths due to preterm birth complications.3

A stable preterm infant in an incubator at JOOTRH, Kisumu, Kenya.

The newborn unit admission/resuscitation room at JOOTRH.
The neonatal mortality rate (NMR) in sub-Saharan Africa is high with an estimated regional NMR of 27.7 deaths per 1,000 live births.4 Although the NMR has decreased, few sub-Saharan African countries are on track to meet the Sustainable Development Goal of NMR of at least as low as 12 deaths per 1,000 live births by 2030. One of the most populous countries, Nigeria, has an NMR of 36 and in Kenya, another LMIC, the NMR is 19.6.4 Attention is focusing on identification of low cost, feasible interventions to address preventable causes of death in LMICs in high-risk preterm and LBW newborns.
Despite the high economic burden and clinical significance of prematurity, there is a paucity of data regarding the morbidity pattern of premature neonates in developing countries.5 Little is known about their postnatal growth outcomes, and even less about what is being done to meet their increased nutritional requirements. In Uganda, for example, a retrospective study at a rural faith-based hospital, using in-patient records of preterm infants for a one-year period (July 2017 to June 2018) revealed that nearly three quarters of them had postnatal growth failure (discharge weight less than the 10th percentile of the expected intrauterine growth for the same postmenstrual age).6 Delayed initiation of enteral feeds and sepsis were highly associated with postnatal growth failure. Early initiation of enteral feeds as soon as possible in these infants was recommended, but no clear guidelines were put forth.
Neonatal networks, including electronic linkage of clinical databases, are critically important platforms for documenting outcomes and improving care for preterm infants.7 Although a recent review identified 82 national or regional databases, none of these were in sub-Saharan Africa.8 This highly informed the decision, in 2018, to form a core network of seven neonatal units (NNUs), five in Nigeria and two in Kenya, in collaboration with the Liverpool School of Tropical Medicine to establish a neonatal nutrition network, NeoNuNet, in sub-Saharan Africa (TABLE 1). NeoNuNet’s vision is for these seven NNUs to work together, sharing expertise and experience to improve clinical outcomes of preterm and LBW infants across the region.
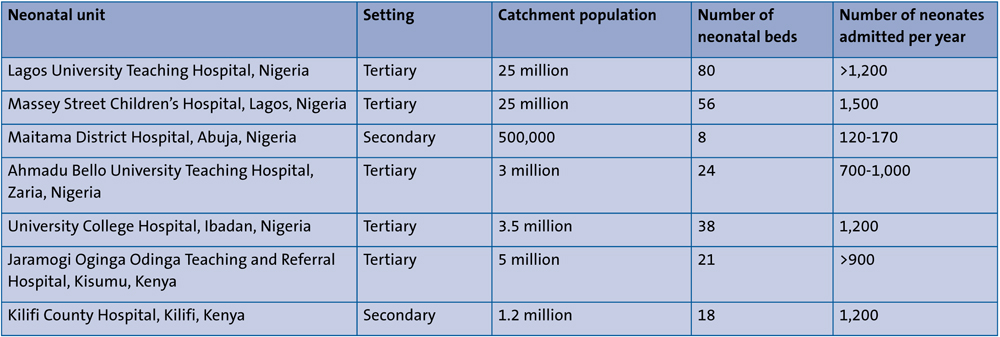
TABLE 1 NeoNuNet: the NNUs working in collaboration with the Liverpool School of Tropical Medicine in sub-Saharan Africa.
NeoNuNet: activities
NeoNuNet activities started in March 2018 at the annual meeting of the Nigerian Society of Neonatal Medicine in Ibadan. Over 60 neonatologists, paediatricians, specialist nurses and NeoNuNet guests from the UK and Kenya took part in a two-day meeting of presentations on neonatal care in low resource settings. Attendees conducted a survey of neonatal feeding practices in their units and also participated in choosing a set of neonatal core outcomes (FIGURE 1).

FIGURE 1 Group work: choosing a set of neonatal core outcomes at the annual meeting of the Nigerian Society of Neonatal Medicine in 2018.
In June 2018 Nigerian and UK NeoNuNet collaborators attended a meeting in Kisumu for Kenyan stakeholders from the Ministry of Health, Unicef and university teaching hospitals (FIGURE 2). At the workshop, the list of variables for standardised data collection was finalised. The NeoNuNet members also visited the neonatal units in Kisumu and Kilifi.

FIGURE 2 NeoNuNet delegates in Kisumu, Kenya, June 2018.
Achievements to date
Data collection on clinical phenotypes, enteral feeding, growth and outcome at discharge of newborns admitted under the age of 48 hours, was carried out for six months in the seven neonatal units. De-identified data on the 2,280 neonates was entered onto a REDCap database (project-redcap.org) hosted at Liverpool School of Tropical Medicine. Data analysis is ongoing and has so far elucidated the burden of disease of the cohort (manuscript submitted for publication) and the association between time to full enteral feeds, and morbidity and mortality of very low birth weight (VLBW) babies (submitted for publication). Use of standardised forms and growth measurements during this period has also strengthened data collection during history taking in the various NNUs.
An overview of systematic reviews of the evidence informing enteral feeding practices in VLBW babies by NeoNuNet members has highlighted the lack of high-quality evidence from research carried out in, or relevant to, low resource settings in sub-Saharan Africa (submitted for publication). Another study carried out in two of the network NNUs in Nigeria elicited neonatal core outcomes of choice of health workers and parents (in press).
Sample collection
During the same six-month period, the seven NNUs collected high vaginal swabs (HVSs) from mothers during delivery to provide a resource for subsequent analysis of the vaginal microbiome in mothers delivering LBW and VLBW infants in these settings. Thereafter, stool samples were collected from the VLBW infants of the mothers in whom HVSs had been collected to determine the acquisition of antimicrobial resistant genes in the faecal flora. They were also stored for future analysis of the gut microbiome of the VLBW infants.
We have also pioneered innovative techniques to measure micronutrient status in very small blood samples (10-20µL) using the volumetric absorptive microsampling technology, combined with liquid chromatography-mass spectrometry and QPlex Array analysis (Quansys Biosciences, http://quansysbio.com/multiplex/multiplex-assays) through a newly developed multi-channel array plate for assessing inflammatory markers in, and micronutrient status of, VLBW infants. An initial assessment of the reliability of finger/heel-prick samples is being assessed by comparison with the venous samples. Establishing these methods in capillary blood samples would make this novel technique readily available to many population groups in need of micronutrient interventions, including mothers in the assessment of ante-natal nutritional factors on clinical outcomes in infants.
NeoNuNet aims to build capacity in neonatal units in sub-Saharan Africa, some with limited previous research experience, and also engage researchers who are new to working in poorer countries. The network is growing to include members working in Uganda, Rwanda, Ghana, Malawi and Zambia. Current network activities include regular conference calls to share experiences of quality improvement initiatives and plan collaborative research projects. The Ibadan site has been successful in obtaining Medical Research Council (UK) funding for a feasibility study of probiotics administration in VLBW neonates. Pragmatic, large-scale studies of affordable, feasible and safe nutritional interventions are planned for LBW newborns, to include research on longer-term outcomes.
Acknowledgement
The authors would like to offer their special thanks to Dr Alison Talbert for her comments on the manuscript.
Or read this article in our
Tablet/iPad edition
