

The impact of the SARS-CoV-2 pandemic on neonatal care
The SARS-CoV-2 (COVID-19) pandemic emerged in late 2019, sweeping across the globe and leaving a very different world in its wake. All healthcare systems had to adapt with little warning to a potentially overwhelming risk. Neonatal units (NNUs) were no exception despite COVID-19 being predominantly a disease of adults.
Liz McKechnie1
Consultant Neonatologist
l.mckechnie@nhs.net
Kirsteen MacSween2
Foundation Year 2 Doctor
Caroline Fraser1
ST5 Paediatric Trainee
Tracy Clinton2
Senior Charge Nurse and FICare Co-ordinator
Dawn Clements1
Family Care Sister
Neil Patel2
Consultant Neonatologist
neilpatel1@nhs.net
1Leeds Centre for Newborn Care, Leeds General Infirmary
2Department of Neonatology, Royal Hospital for Children, Glasgow
The SARS-CoV-2 (COVID-19) pandemic emerged in late 2019, sweeping across the globe and leaving a very different world in its wake. All healthcare systems had to adapt with little warning to a potentially overwhelming risk. Neonatal units (NNUs) were no exception despite COVID-19 being predominantly a disease of adults.
Restrictions designed to prevent spread of COVID-19 have profoundly disrupted our usual models of care, particularly the ability of families to care for their baby in the NNU.
This article explores these impacts and describes the innovative ways that neonatal teams have responded in two NNUs that had already embedded models of family integrated care (FICare). We used electronic surveys, completed by over 170 parent and staff respondents between April and July 2020, to identify themes relating to the personal and professional impact and response to the pandemic in our units
COVID-19 and working in the NNU
Most staff reported a negative impact on their work. As COVID-19 hit the UK in March 2020, many practices had to be adapted. In the early days, fast-changing advice and inconsistent communication was difficult. For many staff maintaining morale in the team was also hard. New requirements for use of personal protective equipment (PPE) and face masks were particularly challenging; not only being uncomfortable but affecting communication with families and colleagues. Staff felt that the FICare philosophy of supporting families as confident partners in care was minimised in the early weeks and made more difficult by restrictions of social distancing. There was also increased anxiety about the potential risk of COVID-19 to staff themselves.
Encouragingly, nearly half of staff respondents recognised a positive impact on their work. Teamworking and relationships improved, with increased recognition of each other’s well-being and roles. While traditional methods of teaching and education were missed, the introduction of remote technologies was appreciated, allowing a wider group to benefit.
The effect of COVID-19 on the team
Many respondents reported that while stress levels were high, the resilience and adaptability in the team was enhanced. However, social distancing meant break times were difficult, preventing the usual pleasures of being able to sit with friends and ‘debrief’, and requiring staff to move on quickly to make space for colleagues. High levels of staff absence and redeployment were recognised as putting additional stress on an already stretched workforce.
Staff perceptions of effects on the family
Almost without exception, respondents recognised the strain new infection control measures put on parents. Staff saw parental access restrictions and wearing face masks as the principal factors responsible for reduced quality of FICare. The effects of absent extended family, siblings and peer support alongside the challenges of PPE were also frequently cited. Face masks were felt to particularly affect parent-baby interaction and importantly most staff reported feeling comfortable about parents removing these at the cotside. Staff also felt that reduced parental presence during the pandemic had a negative impact although some reported the positive aspects of no visitors for parents, allowing them time to focus solely on their baby. The absence of the usual face-to-face education and support sessions for parents was also recognised.
Personal challenges for staff during COVID-19
For many staff, their role in maintaining team morale and supporting colleagues was challenging. Juggling home life and work became difficult, particularly with school closures and restrictions on normal leisure activities. FIGURE 1 summarises these personal challenges expressed by staff.

FIGURE 1 The personal challenges of lockdown.
The challenge of being a NNU parent during
COVID-19
Restricted access to their babies has been the greatest challenge for families, although they recognised that access was much better than adult patients had endured. They reported increased stress and anxiety, heightened by a lack of privacy and access to facilities such as parent lounges and expressing rooms. They missed these as escapes from the high stress environment of the neonatal intensive care unit. This led to missing out on peer support and a perception that they were not trusted by staff to do the right thing.
Poor communication and changing guidance around parental access was a source of stress. However, use of social media and notice boards to keep them up-to-date were greatly appreciated.
While finding it unpleasant, parents accepted wearing PPE if it enabled them to be with their baby. However, like staff, many parents worried that it interfered with their interaction with their baby.
Breastfeeding mums suffered due to restrictions on their movement around the hospital and lack of facilities. Some report missing meals entirely and worried that this adversely affected their breast milk supply.
The impact beyond the NNU
Babies, families and staff have been affected outside the neonatal unit too.
Previously bustling postnatal wards are much quieter places to work during the pandemic. Strict ‘no visitor’ policies have undoubtedly come at a price: new mothers lacking the normal support of partners and family or friends. However, rapid adaptation has been seen here too, with women offering each other support and midwives going above and beyond to make the transition into motherhood as easy as possible.
Emotions can run high on the postnatal ward and removing the partner support has heightened this. Small setbacks preventing discharge have often become very upsetting. When babies have a prolonged postnatal stay, some partners’ entire parental leave can be exhausted before they meet their baby in person. However, to mitigate the separation there has been an increase in early baby checks to support early discharge, and an increased use of online resources for families.
Going home during COVID-19
At the start of the pandemic ‘rooming in’ was stopped completely. New parents missed out on the opportunity to learn 24/7 care for their baby, affecting their confidence. As restrictions are slowly lifting, rooming in has returned, but often only for one parent. The other parent, usually the father but occasionally a shielding mother, has been left isolated and lacking the education usually received before discharge.
After discharge the outreach nursing team may have to see babies for longer than normal to bolster the education and support the family could not receive in the NNU. Some parents have refused this support for fear of exposure to coronavirus. GPs and health visitor support has also been reduced. However, our experience is that this has not produced an increase in re-admissions.
While newly discharged families have not had the usual face-to-face support from friends and families, they may feel the benefits of being less busy and more time at home without distractions and visitors.
Adapting to the new normal: responding positively to COVID-19
Both parents and staff have recognised and contributed to positive responses to the pandemic (TABLE 1). Reduced footfall through the units led to calmer, quieter places – better for babies, parents and staff. Teams have come together, often sharing praise that previously may not have been as forthcoming. Adaptability has been remarkable – implementing new guidelines and procedures much more efficiently and an increased awareness of infection prevention.
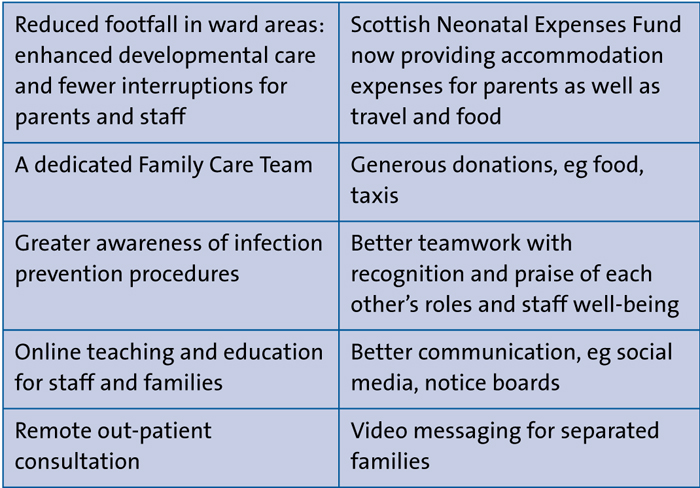
TABLE 1 Some positive outcomes from COVID-19 in NNUs.
Staff have become more aware of the effects of a neonatal journey on families. They have recognised the new stresses for families and provided increased support. There is also increased recognition of, and support for, staff well-being including creating new space for socially-distanced breaks.
The challenge of consistent communication was recognised early in one unit and a daily NNU update bulletin was created, summarising current restrictions and available support (FIGURE 2). These updates were posted throughout the unit and shared widely on social media pages, with a positive response from staff and patients, as well as other units that adapted the idea.
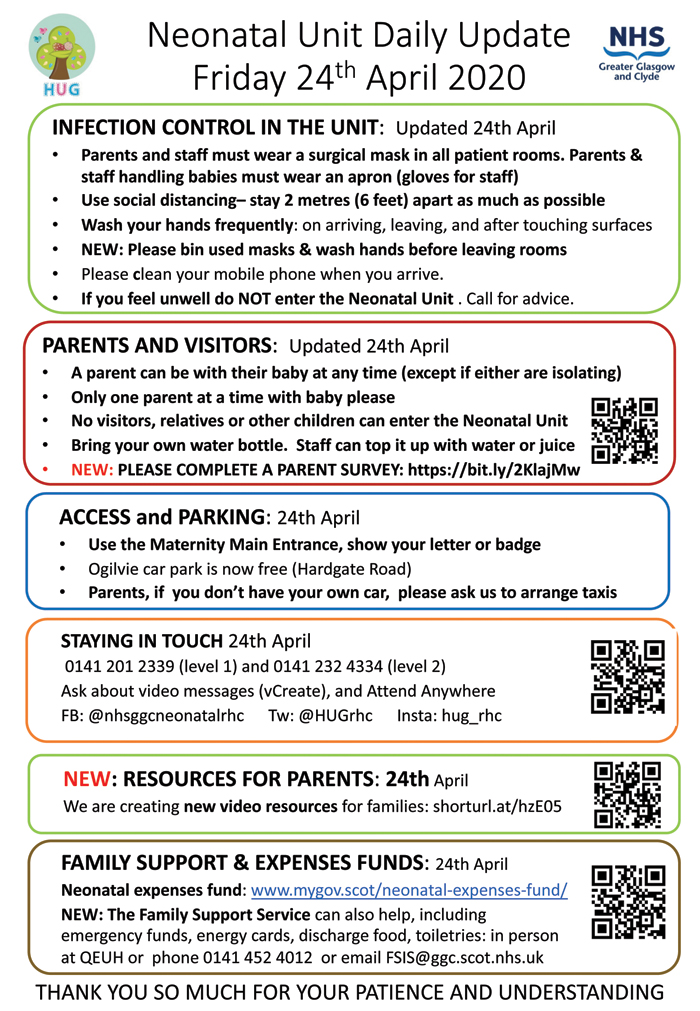
FIGURE 2 The neonatal unit daily update sheet – a simple but effective tool for communicating with staff and families during COVID-19.
A big positive has been the accelerated use of technology – including use of social media to share information and positive messages quickly and consistently for both families and staff, through open and closed groups. The ‘Meet the Team’ daily updates on one unit’s social media pages have been a very popular and positive distraction from COVID-19, introducing a new staff member each day, and giving colleagues and families an opportunity to positively acknowledge them.
Video technologies, including short recorded video platforms such as vCreate, were felt to be a lifeline by families (FIGURE 3). Although both units were early adopters of vCreate, use of this service has increased significantly. As parents and staff recognised the importance of maintaining contact with the wider family, photograph and video use expanded. Video recordings of teaching and education for parents have also been developed and are available to them on their vCreate account. Online resources, such as DadPad and breastfeeding support have also been widely used.

FIGURE 3 A video messaging service for families.
The use of video conferencing technologies for staff, such as Zoom and Teams, has ensured departmental meetings and teach-ing can continue and created new opportunities to connect and collaborate with colleagues locally, nationally, and internationally.
The use of technology for outpatient consultations has also transformed practice. Telephone and video consultations that had been discussed for years were rapidly embedded in practice. Feedback has been broadly positive, though some families and clinicians have missed the reassurance of a face-to-face consultation.
Staff have also adapted their roles to meet the new challenges. In one of our units, nursery nurses volunteered to become part of a new Family Care Team, with a wide remit to support families. They provide emotional, psychological, financial support and signposting, as well as support with breastfeeding and developmental care, relieving some of the stress for new parents and staff. The team has also provided virtual sibling support and sibling packs. They keep in touch by telephone with parents unable to visit daily. Expectant parents, no longer able to look around the NNU before their baby is delivered, are offered a video tour of the unit – available on vCreate. The positive effect of this on families and staff has been significant; going forward we hope to embed the Family Care Team as part of the establishment.
Help has also come from outside. A local taxi service donated a free journey for parents travelling to and from the hospital each day – helping financially and negating the risk of public transport. In Scotland, the universal Neonatal Expenses Fund pays for parents’ travel, meals and now additionally for accommodation, when required. Well-wishers and staff have also ensured that the units are well supplied with food and drinks; we have not gone hungry and have felt the love and support of our wider communities and friends.
Conclusion
The SARS-CoV-2 pandemic has brought about many challenges to neonatal services. Communication, restricted parental access and the discomfort of wearing PPE have been highlighted. However, positives have also been seen with better teamworking, infection control practices and a greater awareness of each other’s well-being. We have embraced technology and new ways of working.
Practices and teams have had to adapt but have done so rapidly, using readily available resources and innovative ideas. Many of these will be taken forward into the post-COVID era further increasing the quality of FICare.
Or read this article in our
Tablet/iPad edition
