

Mortality data by day of life: should this be part of parental counselling on the neonatal unit?
Antenatal counselling given to women and families who are anticipating extremely premature delivery of their baby inevitably involves discussion around mortality and these discussions continue on the neonatal unit. This can be challenging to address, particularly as mortality risk changes over time. Through analysing mortality rates by day of life for each gestation over time in a single unit, it is possible to have more accurate data on this. However, whether or how this should be communicated to parents remains challenging.
Jennifer SalvanosMBChB, BSc, MRCPCH, PGDip
Paediatric Registrar
Jennifer.salvanos@nhs.net
Anne E. Bean
MBChB, MRCPCH, PGDip
Neonatal Registrar and Leadership Fellow
Simon J. Clark
BM, MSc, MRCP, FRCPCH, MD
Consultant Neonatologist
Neonatal Unit, Jessop Wing, Sheffield Teaching Hospitals NHS Foundation Trust
Mortality is often discussed during antenatal counselling with women and their families who may be expecting to deliver at an extremely preterm gestation. It is virtually impossible to provide precise individualised counselling antenatally due to the great many variables applicable to each fetus. The challenge to provide accurate information is exacerbated by mortality data that are generally historical and use national or international statistics that may not apply to an individual population. This becomes even more difficult if the infant is admitted to the neonatal unit, when previously estimated chances of survival may likely no longer be applicable and their chance of mortality at birth is significantly different to their risk if they survive the first few days or weeks.
In the UK, the figures that are most often used are older national figures from the EPICure 2 study in 2006.1 These numbers unavoidably do not reflect more recent advances in neonatal medicine, nor consider variation between neonatal units. The 2019 British Association of Perinatal Medicine (BAPM) Framework for Practice on the management of extreme preterm infants2 gives more up-to-date mortality figures, but it does not consider changes in mortality by day of life once admitted to the neonatal unit. Parents may frequently recall statistics they may have been given during antenatal counselling. However, these are often no longer relevant with increasing days of survival.
By analysing local mortality data by day of life specifically, both antenatal and ongoing counselling of parents and families could potentially be updated and more individualised. The data could also be used to create updated parent information leaflets, if found to be beneficial, as information given during antenatal counselling can be difficult to retain.
Methods
Mortality data were retrospectively reviewed for all babies born between January 2011 and December 2017 at the Jessop Wing level three neonatal intensive care unit (NICU) in Sheffield using the BadgerNet database. The Jessop Wing has approximately 7,0003 deliveries per year and provides intensive care for medical and surgical conditions but does not have facility for cardiac surgery or ECMO (extra corporeal membrane oxygenation). Local policy is that all infants <27 weeks’ gestation or <800g should be delivered and initially cared for at a level three NICU.
Data were collected and analysed on gestation, birth weight, date of birth, length of stay, sex, and survival to discharge. Simple proportions and means were calculated with 95% confidence intervals and Fisher’s exact test was used for categorical variables.
Results
Across the study period, 403 infants of <27 weeks’ gestation were admitted to the neonatal unit. Of these infants, 129 died (32%). The mortality rate was 39/52 (75%) if <24 weeks’ gestation and 90/351 (26%) if born 24-27 weeks’ gestation. The mean birth weight of the cohort was 770g and 56% of the infants were males. The mean length of stay in the neonatal unit prior to death or discharge was 48 days, with 90% of deaths occurring before day 30. There was no statistically significant improvement in gross mortality over the time period.
FIGURE 1 shows that on day 1 of life the probability of being discharged alive for infants born at <27 weeks’ gestation was nearly 70%. This probability significantly rose to 79% by day 4 (p=0.0024). If an infant survived to day 13 the probability of live discharge rose to 84% (p=0.0001) and the prospects of live discharge significantly rose again to 90% if the infant was alive by day 30 of life. The graph also shows a slight increase in mortality if the infant is still in the neonatal unit after day 90 of life. The numbers in this group are small and they may have congenital abnormalities or surgical complications that have led to the prolonged admission and increased mortality risk.
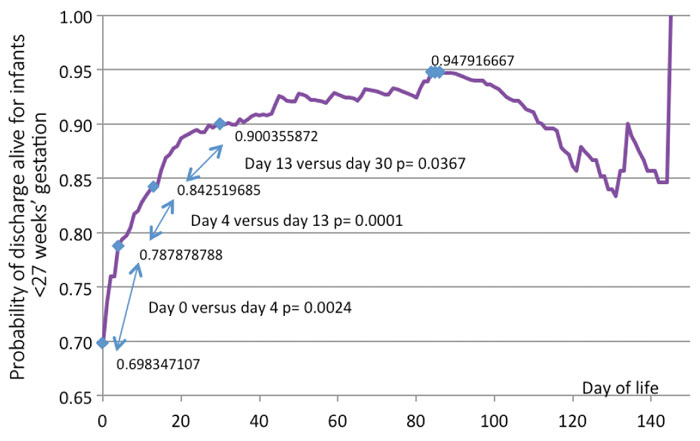
FIGURE 1 Daily change in probability of live discharge for all infants born at <27 weeks’ gestation.
FIGURE 2 expands on the data by showing the probability of live discharge specific to each gestational age. As can be seen, the survival for infants born at 23 weeks’ changes dramatically over the first few weeks of life. This information could be used to help parents cope better with the uncertainties of neonatal care and support increasing optimism over time. An antenatal discussion with parents of a 23-week gestation infant would paint a much poorer picture of prognosis than a discussion with those same parents when the infant has been in intensive care for a few weeks.
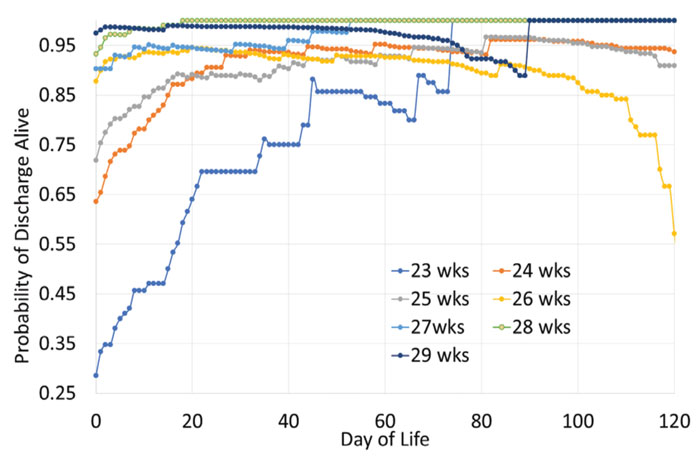
FIGURE 2 Daily change in probability of live discharge for infants born at <30 weeks’ gestation by gestational age.
Discussion
The information extracted from this study can be used to develop a moving proba-bility of survival graph based on gestation and current day of life for extremely preterm infants. This information could be shared with families, both during antenatal counselling and as appropriate when time progresses on the neonatal unit. But, in what way this should be done and to what degree is unclear. FIGURE 3 gives some of the opinions of experienced local clinicians in how they might interpret the data and potentially use it when counselling parents and families.
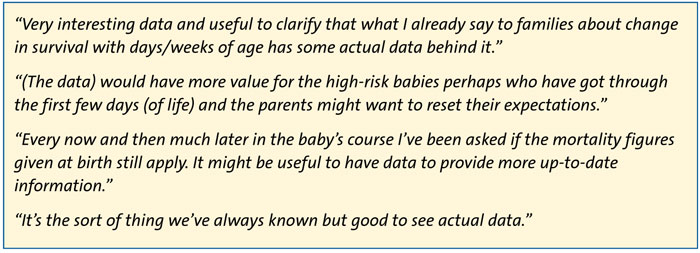
FIGURE 3 Some opinions of clinicians on how they might interpret the data and potentially use it when counselling parents and families.
It is right to emphasise that this information would form only part of much more detailed and specific discussion with parents for their baby. It is important to recognise also that even with regularly updated and unit-specific mortality data, it is impossible to predict accurately the outcome for an individual baby. The ability to communicate that uncertainty to parents is a skill that those working within neonatal care must continually strive to develop.
More research is clearly required, not only to see if this pattern of survival is consistent across other NICUs but also to explore the most effective ways of communicating this information to carers. While it is important that parents and carers are given information in a clear and unambiguous fashion, this should also be accessible and easy to understand. For clinicians, explaining to parents that their child is likely to have a daily change in their probability of survival could be very challenging and poses the questions for future investigation of how this should be best done.
Or read this article in our
Tablet/iPad edition
- Mortality risk varies greatly by day-of-life for extremely preterm infants.
- Parents have a right to accurate and
- up-to-date information, but it is unclear how this should be communicated.
- Including changing mortality rates over time in regional and national information leaflets for parents of extremely preterm infants could be considered.
