

COVID-19: the importance of healthcare professionals in protecting human milk and breastfeeding
It is clear that the world will never be the same since the onset of the COVID-19 pandemic. Our daily routines and the healthcare system will be forever changed. Nonetheless, families will continue to conceive and bring new lives into the world. Now more than ever, families need access to evidence-based lactation care and support. With social distancing there are both opportunities and risks: opportunities to improve breastfeeding outcomes; risks that families may not be able to access much-needed lactation care or lactation technology.
Diane L. Spatz
PhD, RN-BC, FAAN
Professor of Perinatal Nursing and the Helen M. Shearer Professor of Nutrition, University of Pennsylvania
Nurse Scientist for the Lactation Program and
Founder of Mothers’ Milk Bank, Children’s Hospital of Philadelphia
spatz@nursing.upenn.edu
It is clear that the world will never be the same since the onset of the COVID-19 pandemic. Our daily routines and the healthcare system will be forever changed. Nonetheless, families will continue to conceive and bring new lives into the world. Now more than ever, families need access to evidence-based lactation care and support. With social distancing there are both oppor-tunities and risks: opportunities to improve breastfeeding outcomes; risks that families may not be able to access much-needed lactation care or lactation technology.
Guidance from the Royal College of Obstetricians and Gynaecologists (RCOG) and the Royal College of Midwives (RCM) supports the use of human milk and breastfeeding.1 The Royal Colleges report that, to date, the virus has not been found in human milk and that the main risk for COVID-19 transmission is the close contact of the mother and child – an infected mother could transmit the virus via infective droplets. In light of the current evidence, RCOG and RCM state that the benefits of breastfeeding outweigh any potential risks of transmission of the virus through human milk and recommend the following precautions to limit viral spread to the baby:1
- wash hands before touching the infant, breast pump or bottles
- avoid coughing or sneezing on the infant during breastfeeding
- consider wearing a fluid-resistant surgical face mask, if available, while feeding or caring for the baby
- consider asking someone who is not infectedto feed expressed milk to the infant
- if the mother is expressing milk in a hospital, a dedicated breast pump is recommended and the mother should be given explicit instructions for hand washing and pump cleaning/disinfection.
What can healthcare professionals do?
Given the guidance to protect human milk and breastfeeding during the COVID-19 pandemic, the model that I developed to promote and protect human milk and breastfeeding in vulnerable infants is highly applicable (
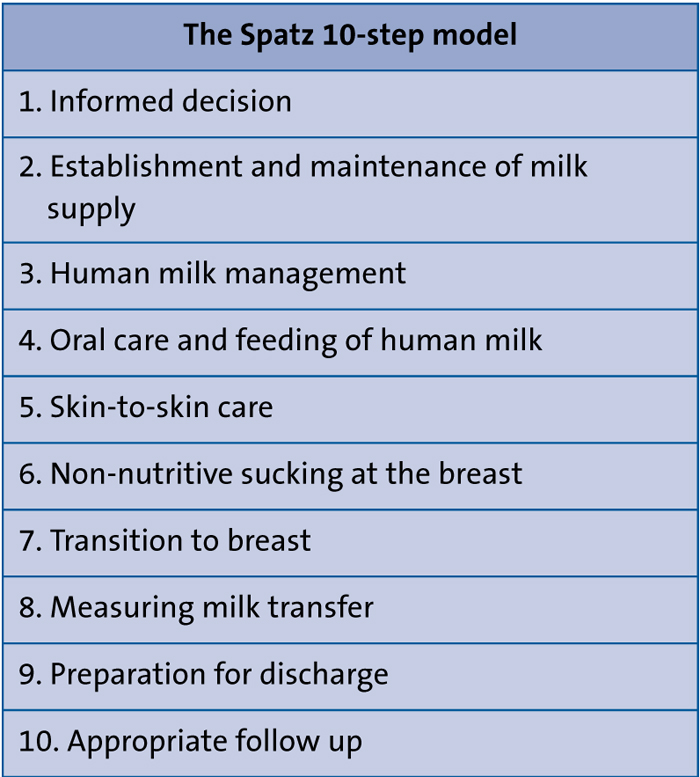
TABLE1 Ten steps to promote and protect human milk and breastfeeding in vulnerable infants.
Step 1: Informed decision
Not all families in the UK and globally have the opportunity to make informed feeding decisions. Many families do not initiate breastfeeding due to a lack of family support, culture and/or lack of education. During this current pandemic, we have the opportunity to change the prenatal care paradigm to ensure that all families make an informed feeding choice.5 Breastfeeding should be a point of discussion at every single prenatal visit.5 At the first point of contact we should assess the family’s exposure and experience with breast-feeding, as well as any positive or negative views. We should provide data and resources to help families understand how and why human milk and breastfeeding are important for their personal situation. In particular, during this pandemic, we can provide information about how human milk protects against other viral infections. Liang and colleagues found that multiple human viruses were more abundant in stool samples from infants who were exclusively formula fed com-pared to those that received either partial or exclusive human milk diets.6
Step 2: Establishment and maintenance of milk supply
During pregnancy, the family should be instructed on the physiology of lactation so that they can have the best opportunity to effectively establish and maintain a milk supply.2-5
The mother begins to secrete milk in the second trimester of pregnancy so regardless of whether she has a preterm or term delivery, her breasts are prepared to make milk for her child. In addition, we should proactively empower the partner/support person so that the mother’s main focus after delivery is to eat, sleep and make milk for the infant.
With the COVID-19 pandemic, some hospitals are separating COVID-positive mothers from their infants immediately at birth. If this is the practice, the mother must be supported to pump early and pump often with a hospital-grade pump.7 Research demonstrates that the sooner the mother expresses after birth (within six hours but ideally within the first hour), the more likely she is to come to volume and have a higher milk supply at three weeks postpartum.8,9 It is particularly important to note that personal-use pumps are not designed to initiate lactation.10 Mothers who are separated from their infants at birth for any reason should have access to a hospital-grade pump with ‘initiation technology’.10,11
There is a critical window of opportunity for the establishment of milk supply and therefore the role of the paediatric healthcare provider is of paramount importance.11 Some hospitals discharge mothers and their infants early (within 24 hours of vaginal birth and 48 hours of caesarean birth) so it is essential that at the newborn visit the provider determines if the mother has effectively converted from lactogenesis I to lactogenesis II. Mothers may continue to need in-person technical assistance for breastfeeding but should also be referred to virtual support groups and ‘tele-lactation’ visits.
Step 3: Human milk management
Step 3 of my model is of critical importance during the pandemic for several reasons. First, if mother and child are separated and the mother is expressing milk, she and her family need specific instructions on daily cleaning and disinfection of the pump, the pump pieces and the pump kit.1 The family will also need instructions on correct storage of the milk, with an emphasis on the use of freshly expressed milk.2,3 Human milk contains live white blood cells (WBCs), stem cells, lactoferrin, antioxidants, antibodies, and other immune, growth, and developmental factors.5 When milk is frozen, WBCs and stem cells are destroyed and many of the other immune components become less potent. Fresh milk matters now more than ever.
So many unknowns…
With the COVID-19 pandemic, there are many things that we are unable to predict and control. We don’t know when this pandemic will end or when social distancing guidelines will relax but what we can embrace is human milk and breastfeeding as a life-saving medical intervention. FIGURE 1 demonstrates just how vital human milk is. Baby Charlotte was born with a giant omphalocele (exomphalos) that had been prenatally diagnosed. I met with her mother while she was pregnant and provided her with a personalised 1:1 consultation.5 Her mother followed the Spatz 10-step model exactly as instructed. She produced over a litre of milk per day and had not only enough milk for her daughter, but was able to donate milk to a non-profit milk bank. Charlotte will be 10 this year and has no health concerns. Her photos are a testimonial to the life-saving power of human milk as a medical intervention.

FIGURE 1 The life-saving power of human milk: first time at the breast
for baby Charlotte who will be 10 years old this year (below).

FIGURE 2
Or read this article in our
Tablet/iPad edition
