

National research to understand and better manage neonatal COVID-19
The novel coronavirus SARS-CoV-2 was identified in late December 2019 and causes coronavirus disease (COVID-19). This disease has been declared a pandemic by the World Health Organization and is an international public health crisis. So far there is only relatively limited information describing the incidence, clinical course, treatments or outcomes of SARS-CoV-2 infection and COVID-19 in neonates up to 28 days old.
The Neonatal Complications of COVID-19 Surveillance GroupChris Gale Reader in Neonatal Medicine, Imperial College London
christopher.gale@imperial.ac.uk
Marian Knight Professor of Maternal and Child Population Health, University of Oxford
Shamez Ladhani Consultant Epidemiologist, Public Health England, Colindale
Elizabeth Draper Professor of Perinatal and Paediatric Epidemiology, Department of Health Sciences, University of Leicester
Don Sharkey Associate Professor of Neonatal Medicine, University of Nottingham
Cora Doherty Consultant Neonatologist, University Hospital of Wales, Cardiff
Helen Mactier Neonatal Consultant and Honorary Clinical Associate Professor, Princess Royal Maternity and University of Glasgow
Jennifer Kurinczuk Professor of Perinatal Epidemiology, University of Oxford
There are three main ways that neonates may be affected by SARS-CoV-2 infection:
- Potential vertical transmission of SARS-CoV-2 from mother to infant during pregnancy, labour or birth which may lead to neonatal COVID-19.
- Horizontal transmission of SARS-CoV-2 in the neonatal period; this may also lead to neonatal COVID-19 and can occur from close family contacts such as the mother, or from nosocomial transmission in places such as neonatal units.
- Maternal COVID-19 that impacts pregnancy or labour and birth, leading to neonatal complications such as preterm birth. Such circumstances can be thought of as indirect neonatal effects of maternal COVID-19, and will include situations where the neonate does not contract SARS-CoV-2.
Understanding how common each of these different scenarios are is critical to prevent and control neonatal COVID-19, and to plan neonatal services to best cope with the pandemic. Understanding vertical and horizontal transmission will help protect neonatal staff and those attending births, as well as informing management of babies born to women with COVID-19. Accurate data describing the presentation and clinical course of neonatal COVID-19 are important to determine which infants might benefit from current supportive treatments, and to identify where potential disease modifying treatments might be tested in clinical trials. Data describing the direct and the indirect neonatal effects of COVID-19 are also needed to predict and plan neonatal care effectively, particularly as SARS-CoV-2 may lead to increased preterm birth or other birth-related compli-cations, similar to previous pandemic respiratory viruses like 2009/H1N1 influenza.1
At time of writing there is no definitive evidence of vertical transmission of SARS-CoV-2; so far cases suggesting vertical transmission have been limited to a small number with increased IgM levels in umbilical cord samples,2,3 but the validity of these tests is not certain.4 Data describing how common COVID-19 is in the neonatal period come from single centre studies5 or from healthcare systems like China,6 which have taken a different approach to perinatal management of SARS-CoV-2 infection than that currently recommended in the UK.7 These countries have implemented almost universal caesarean birth followed by strict and prolonged isolation of the newborn from the mother and other affected family members. Unfortunately, there is no good evidence to guide any current practice following birth to a mother with COVID-19. The clinical course of paediatric SARS-CoV-2 infection and COVID-19 in older babies and children is slightly better described and appears to be considerably less severe than in adults, but more recent data6 suggest that up to 10% of neonates and infants with COVID-19 develop severe or critical disease. It is, however, unclear how generalisable these data are to UK paediatric and neonatal practice given the different perinatal and neonatal management practices.
The wider impact of maternal COVID-19 on babies is also not fully understood; while several hundred women with COVID-19 in pregnancy have been described worldwide, these are mainly in limited case series or single centre studies. The majority of reported newborn infants were asymptomatic for COVID-19 but several were born preterm, and at least one baby who died in the neonatal period has been reported – suggesting that indirect impacts of maternal COVID-19 on neonatal services may be substantial in the context of sustained community transmission.
In the absence of reliable and relevant data we urgently need active population-based surveillance data to inform UK neonatal care. Such data differ from information collected through registries, which are commonly retrospective and may not achieve universal coverage, and as a result registry data cannot be guaranteed to provide robust or reliable information about incidence or complication rates at the population level. The British Paediatric Surveillance Unit (BPSU) has pioneered population-based active surveillance for rare diseases since 1985. The Orange Card system developed by the BPSU has been an exemplar for national surveillance systems in other specialties and internationally. Crucially, the BPSU emails paediatricians and neonatologists across the UK and Ireland every month and asks them to report whether they have managed a baby or child with any condition listed under active BPSU surveillance. Following each positive response, the paediatrician is sent a detailed questionnaire to complete. Active surveillance prompts a response even if no babies or children were managed by the reporting doctor; because more than 90% of paediatricians and neonatologists respond to the BPSU every month this ensures high case ascertainment and enables population incidence rates to be estimated.
A BPSU study entitled Neonatal Complications of Coronavirus Disease (COVID-19) started on 1 April 2020 to ascertain robust data on incidence, clinical course and management of any neonate affected by COVID-19 from 1 March 2020 onwards, and has been identified as an Urgent Public Health Priority study by the NIHR Clinical Research Network. Any baby or infant that meets the surveillance case definition (TABLE 1) should be reported to the BPSU. Because of the unprecedented nature of the COVID-19 pandemic, for the first time the BPSU is asking for notifications of affected babies to be reported weekly rather than monthly. To ensure that all affected babies are identified as completely as possible the study will also link with other related data sources including ongoing United Kingdom Obstetric Surveillance System (UKOSS) surveillance of COVID-19 in pregnancy for maternal cases, MBRRACE-UK (Mothers and Babies: Reducing Risk through Audits and Confidential Enquiries across the UK) for neonatal deaths and stillbirths, and Public Health England (PHE), Health Protection Scotland, Public Health Wales and the Health and Social Care Public Health Agency in Northern Ireland. To limit the amount of information that neonatologists and paediatricians are asked to report and to further increase case ascertainment, surveillance will also link with routinely recorded neonatal and paediatric intensive care data held in the National Neonatal Research Database (NNRD) and Paediatric Intensive Care Audit Network (PICANet). The resulting data will be used to inform clinical care and service provision and to advise pregnant women. It will also be shared with global registries for international comparisons.
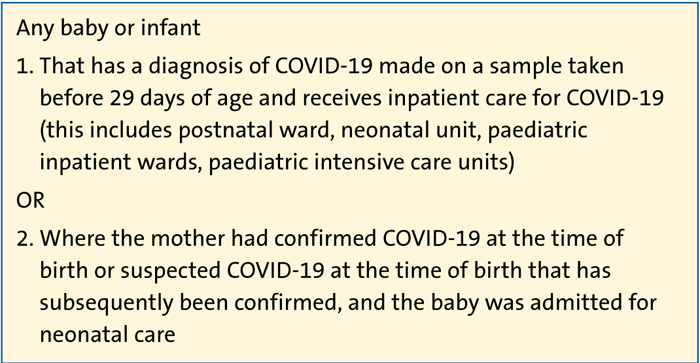
TABLE 1 BPSU surveillance case definition for neonatal complications of COVID-19.
There are some limitations to the data that will be obtained from BPSU surveillance of COVID-19 as babies reported will only be those seen in secondary and tertiary care. It will therefore miss babies who are asymptomatic or with milder infections developing in the community. Because testing to date has been recommended for clinical indications only, it is unlikely to obtain the early antigen and serological samples needed to delineate fully between vertical and horizontal transmission. The most recent Royal College of Paediatrics and Child Health (RCPCH) guidance addresses this matter to some degree, in suggesting that early testing, if available, may have utility in helping to understand perinatal SARS-CoV-2 infection. We note that such testing is also commonly practised across the world.
The periCOVID study (www.pericovid.com) recently established at St Georges Hospital in collaboration with PHE will help us to better understand perinatal SARS-CoV-2 transmission.
To determine which treatments may improve outcomes in neonatal COVID-19 randomised trials of interventions have been rapidly developed, including the Randomised Evaluations of COVID-19 Therapy (RECOVERY) trial (www.recoverytrial.net), which can enrol pregnant women and children, including neonates.
Although neonates, infants and children appear more mildly affected by COVID-19 than adults, robust population level data are limited, and considerable uncertainty remains about the incidence, transmission, clinical course and outcomes of neonatal SARS-CoV-2 infection and COVID-19, and the impact of maternal COVID-19 on the newborn. National research and active surveillance through established national systems such as the BPSU are the simplest, quickest and most efficient way to obtain accurate data to inform optimal neonatal care in the context of the SARS-CoV-2 pandemic. Data from this surveillance project will be rapidly and regularly summarised and provided to key stakeholders, such as the British Association of Perinatal Medicine (BAPM) and the RCPCH, to provide updates on the impact of COVID-19 in the neonatal population, allowing timely review and dissemination of guidance during the emergence of this new disease.
Or read this article in our
Tablet/iPad edition
