

A neonatal short-term home nasogastric tube feeding programme
Every neonatal unit will be familiar with a cohort of mid to late preterm babies who are otherwise well but spend the last few weeks of their admission establishing sucking feeds. These babies can spend several days to weeks weaning off nasogastric tube (NGT) feeds after they have been deemed medically ready for discharge. A solution to help speed up discharge for these babies is a short-term home NGT feeding programme. This article looks at the experiences and outcomes over the first five years of setting up a short-term home NGT programme on the neonatal unit at John Radcliffe Hospital.
Katherine Wood1
BMedSci, BMBS, MRCPCH, Neonatal Registrar
Frances O’Brien1
BSc, MBBS, MRCP, DRCOG
Karen Liddle1
RGN, Neonatal intensive care course (405), Neonatal Outreach Lead
Rhys Dore2
BABMBCh, Foundation Year 2 Doctor
1Neonatal Unit, John Radcliffe Hospital, Oxford
2Brighton and Sussex University Hospitals NHS Trust
The basis for home NGT feeding programmes has been in existence since the 1980s1 and has been described as not only having cost and resource benefits for neonatal units but also psychological, developmental and practical benefits for the infants and their families.2,3 Additionally, it has been shown that babies who are discharged with NGT feeds at home have a reduction in clinical infections with no significant increase in re-admission rates or difference in weight gain, compared to those establishing feeds in hospital.4
Origins of the programme
John Radcliffe is a level 3 neonatal unit in the Thames Valley Neonatal Network. It consists of 14 intensive care beds, 11 high dependency beds and 22 low dependency beds with four ‘homeward bound’ rooms (allowing parents to room in with their baby prior to discharge).
In 2012 a commissioning quality and innovation (CQUIN) goal was set up in the neonatal unit to identify babies with a gestational age of less than 36 weeks who may be suitable for short term NGT feeding at home while establishing breast or bottle feeding, and to provide a comm-unity outreach service to allow this to happen.
A programme was therefore set up to target babies born at 28-35+6 weeks’ gestation. The criteria for babies and families to be discharged on the home NGT programme were set out (TABLE 1). These criteria evolved as the programme was established and different obstacles were encountered. For example, one mother assessed for the programme was colour-blind due to retinopathy, so she was unable to interpret the colours on the pH testing strips. Therefore, extra family criteria were added to address this potential safety issue.
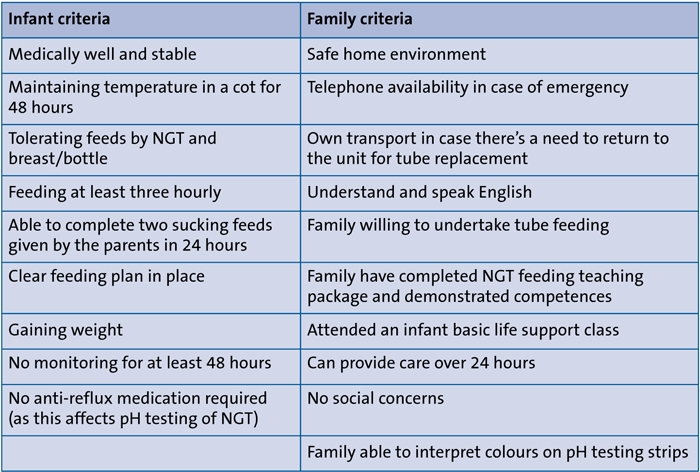
TABLE 1 Infant and family criteria for discharge with an NGT.
A detailed training package and competency list was developed to ensure that the parents had the full set of necessary skills to manage their baby with an NGT at home. A flow diagram was developed to help guide hospital staff in the event of parents telephoning the neonatal unit for advice out of hours (when the outreach team was unavailable) if a baby was not sucking well or appeared unwell (FIGURE 1).
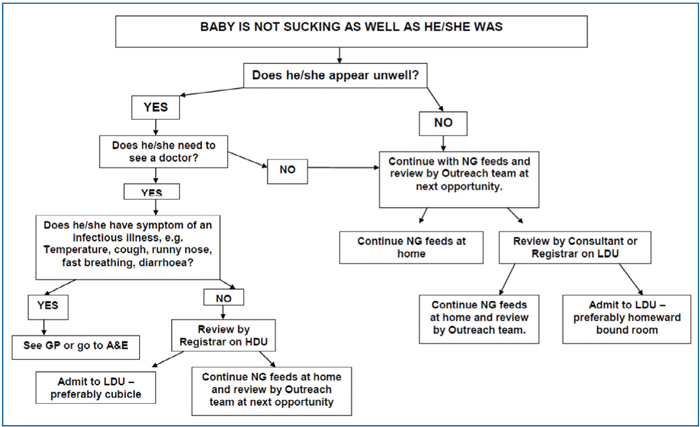
FIGURE 1 Flowchart for the baby who is not sucking as well as he/she previously was.
Initially the team involved in setting up the programme included:
- two existing neonatal outreach nurses (band 7 at 1.9 whole time equivalent)
- an existing discharge co-ordinator (band 6 at 36 hours/week)
- two existing band 6 neonatal nurses (2.0 whole time equivalent) on a six-month secondment.
The neonatal nurses worked with the outreach team as well as taking telephone consultations on the unit. Additionally, a neonatal consultant was allocated 1 PA with existing administrative support (band 3 at 0.3 whole time equivalent).
As the programme became established and grew, the supporting outreach team expanded and now consists of two band 7 nurses and an additional band 6 nurse (totalling 2.8 whole time equivalent). The consultant support is now provided by the existing attending low dependency consultant.
The payment schedule for setting up the CQUIN in the first year stipulated that in each quarter 25% of value would be given providing the following targets were met:
- quarter 1: confirmation of set up for collection of data
- quarter 2: 20% of the eligible patient group receiving tube feeding at home
- quarter 3: increasing to 25% of eligible patient group
- quarter 4: 30% of eligible patient group.
After these targets were reached the same data were provided for two more years before funding was secured for the long term.
A summary of what went well during the programme set up, along with the challenges and some tips for running a similar programme can be seen in FIGURE 2.
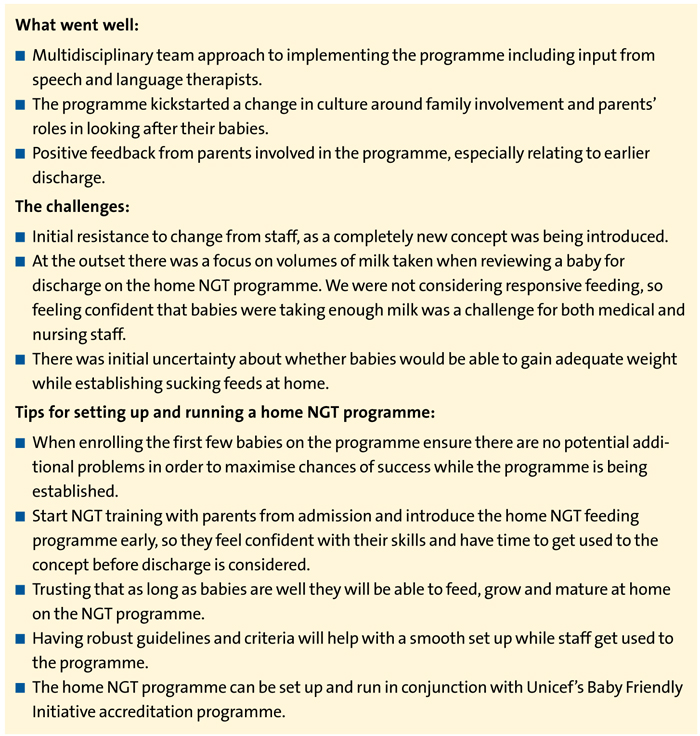
FIGURE 2 A summary of what went well and the challenges encountered during set up, and some tips for running a home NGT programme.
Summary of the reviewed data
In the first five years after the home NGT feeding programme was established (from 1 April 2013 to 31 December 2017) there were a total of 798 babies born between the gestations 28+0 to 35+6 weeks. This amounted to a total of 20,174 bed days, with gradual increase in bed days each year (TABLE 2). A total of 234 babies have been discharged on the home NGT feeding programme, which is, on average, 32% of babies born at 28+0 to 35+6 weeks’ gestation.
The median corrected gestational age (cGA) at discharge for all babies born between 28+0 and 35+6 weeks’ gestation over the five-year review period was 36+5 weeks. For the babies discharged on the home NG feeding programme, on average this was five days earlier at 36+0 weeks. FIGURE 3 gives a breakdown for each year.
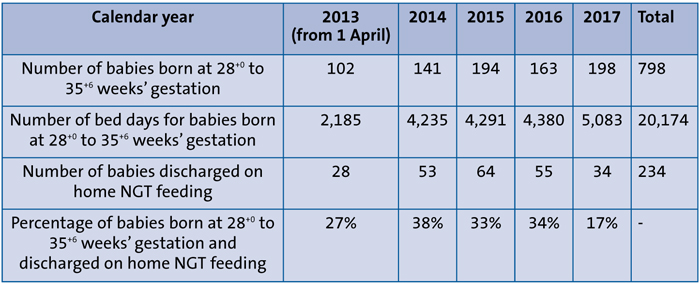
TABLE 2 Number of babies born and number of bed days at 28+0 to 35+6 weeks’ gestation, with number and percentage of babies discharged on the home NGT feeding programme (1 April 2013 to 31 December 2017).
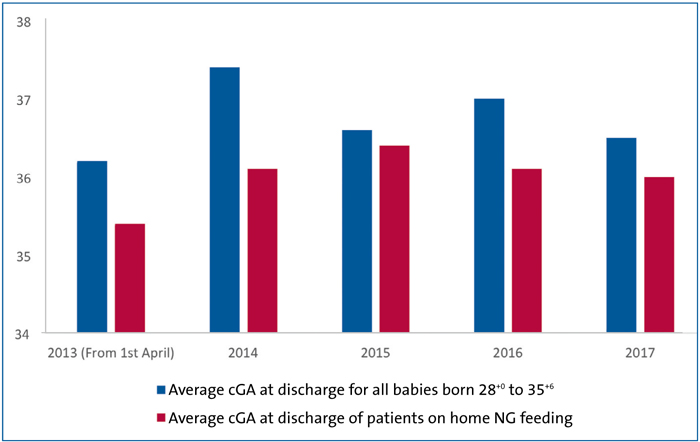
FIGURE 3 Comparison of cGA at discharge of all babies born at 28+0 to 35+6 weeks’ gestation vs those discharged on the home NGT feeding programme (1 April 2013 to 31 December 2017).
Finances
The costs of the home NGT feeding programme were analysed. During the first year of start-up, consultant time at 1 PA was required (cost to the trust estimated at £9,000/year). After the first year this was incorporated into the everyday role of the attending consultant, resulting in no extra costs for the consultant cover. An extra community neonatal nurse was employed after the programme was established (cost to the trust estimated at £45,000/year). Travel reimbursement for the community nurses can be estimated at around £3,000/year. There was no extra cost of consumables (NG tubes, syringes etc) as the babies would have used the same consumables if they remained on the unit.
When the saving of each low dependency bed day is balanced by the cost involved in providing the home NGT programme (including initial start-up and resulting running costs), there has been an estimated net saving of around £994,000 over the first five years (a total of 2,728 bed days saved by discharging babies home earlier on the programme, with a low dependency bed cost estimated at £433 per day5) (TABLE 3).

TABLE 3 Number of bed days saved and estimate of net savings of providing the home NGT programme per year from period of 1 April 2013 to 31 December 2017. *Savings from reduction in bed days minus cost of home NGT programme/year.
Weight gain
Not only has the home NGT programme provided financial benefits but we have also measured objective advantages for the patients. An analysis of a random selection of patients between January 2014 and February 2016 was carried out to look at differences in weight gain between the babies that were discharged on the home NGT programme and equivalent babies eligible (ie no significant ongoing medical problems, no problems with growth and no social concerns) for home tube feeding but who, due to parental choice, stayed on the neonatal unit to establish sucking feeds.
The two groups had no significant difference in gestation, birth weight or feeding method. The analysis showed there was a significantly higher increase in weight gain for babies discharged on the home NGT feeding programme (TABLE 4).6

TABLE 4 Mean weight gain (g/kg/day) in 62 babies on the home NGT feeding programme vs 81 babies establishing sucking feeding on the neonatal unit (January 2014 to February 2016). P value calculated with Mann-Whitney U test.
This suggests the home environment is more conducive to higher weight gains and possible reasons for this include:
- an increase in responsive feeding when parents are by their baby’s side 24 hours a day
- less disturbance for the babies when they’re not in hospital
- maternal stress is likely to be decreased in the home environment, which is associated with an increase in milk production as well as availability.7
Breastfeeding rates at discharge
We compared the percentage of babies born between 28+0 to 35+6 weeks’ gestation discharged breastfeeding on the home NGT programme with those discharged breastfeeding but not on the home NGT programme. We saw consistently higher breastfeeding rates at discharge for babies on the programme compared to those not on it (FIGURE 4). This might suggest that a higher level of involvement of parents in their babies’ care, together with earlier discharge, may result in higher breastfeeding rates. However, we need to be aware that those babies not on the home NGT feeding programme may have additional problems that not only excluded them from being enrolled on the programme but may also have impacted their ability to breastfeed (for example, a more unstable neonatal course with resultant complications of prematurity).
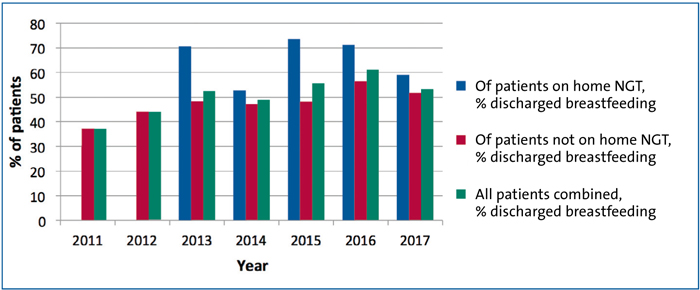
FIGURE 4 Comparison of babies (28+0 to 35+6 weeks’ gestation) discharged breastfeeding in 2011-2012 (prior to establishment of the home NGT feeding programme) and 2013-2017, after the home NGT feeding programme was established.
Impact on families
Some benefits related to early discharge resulting from the home NGT feeding programme are harder to quantify. We can get a sense of the impact on families from the feedback we received, for example, being more comfortable at home and not having to juggle time between coming to hospital and being with older siblings. FIGURE 5 illustrates some of the quotes from parents on the programme.
FIGURE 5 Quotes from parents about the home NGT feeding programme.
Readmissions
We found that over the five years of analysis some babies on the home NGT feeding programme have had to be re-admitted, as might be expected. However, there have been no re-admissions due to faltering growth or problems related to the NGT. Reasons for re-admission include bronchiolitis, requirement for blood transfusion, hernia repair, pyloric stenosis and gastro-oesophageal reflux.
Changes to the home NGT feeding programme over the last five years
As the home NGT feeding programme has developed there have been some changes. The programme has started to accept babies from a lower gestation (ie from 24 weeks’ gestation, providing all the other infant and family criteria are met). In 2017 two babies born at less than 28 weeks (at 24+6 and 26+3 weeks’ gestation) were discharged on the home NGT feeding programme. Both babies saved six days, where they were at home instead of in hospital establishing sucking feeds. Since then, there has been a gradual increase in the number of extremely preterm infants discharged home with NGTs; this inclusion of babies of lower gestation has helped the families that have some of the longest stays on the unit to get home sooner.
Another change is the continuation of breast milk fortifier (BMF) at home. Traditionally BMF has been stopped when babies have been discharged or have been established onto full breastfeeds. BMF ‘boosts’ have been introduced, which involves mixing a 2.2g sachet of BMF in 5mL of warmed breast milk and administering it via a teat four times a day before feeds. This continuation of BMF at home should allow for further enhancement of weight gain.8
Summary and future direction
Over the five-year period reported, we have discharged a total of 234 babies on the home NGT feeding programme, which is equivalent to 32% of all babies born at gestations of 28+0 to 35+6. There have been several objective gains from the prog-ramme, from financial (with estimates of savings of £994,000 over the first five years), to enhancement of growth of babies. We have also seen higher breast-feeding rates and other gains that are harder to quantify arising from earlier discharge (eg enhanced family bonding, increased family involvement and confidence in their baby’s care).
As the programme grows and progresses we aim to develop it further. Future plans include altering infant criteria to allow consideration of those infants being discharged on home oxygen or on anti-reflux medication, which will allow more of our babies to benefit from the programme.
Or read this article in our
Tablet/iPad edition
- We share our experiences of setting up a short-term home NGT feeding programme for well preterm babies establishing sucking feeds.
- The programme has several benefits: reducing hospital stays, enhancing weight gain, increasing breastfeeding rates, significant financial savings, and enhancing family bonding.
Also published in Infant:
