

BAPM Frameworks for Practice: supporting neonatal staff to optimise perinatal care
Last year was an important one for BAPM Frameworks for Practice. An editorial discussing the framework on the management of extreme preterm birth made the front cover of the Lancet and existing guidance on consent with a framework on shared decision-making was updated. BAPM also published a document on determining cot capacity, designed for use alongside the existing framework on service standards for hospitals providing neonatal care. At the time of writing, a framework on preventing and managing dropped babies in hospitals is out for consultation and additional frameworks on therapeutic hypothermia, family integrated care, and management of the difficult airway as well as career pathways for advanced neonatal nurse practitioners are due to be published in 2020.
Kate DinwiddyChief Executive, BAPM
Helen Mactier
President, BAPM
Last year was an important one for BAPM Frameworks for Practice. We made the front cover of the Lancet with an editorial discussing our framework on the management of extreme preterm birth and we updated existing guidance on consent with a framework on shared decision-making. We also published a document on determining cot capacity, designed for use alongside our existing framework on service standards for hospitals providing neonatal care. At the time of writing, a framework on preventing and managing dropped babies in hospitals is out for consultation and additional frameworks on therapeutic hypothermia, family integrated care, and management of the difficult airway as well as career pathways for our cherished advanced neonatal nurse practitioners (ANNPs) are due to be published in 2020.

All BAPM Frameworks for Practice are written on a voluntary basis by BAPM members, generally with additional input from a variety of experts and relevant organisations. Following several face-to-face and/or virtual meetings, a working group with relevant expertise produces a first draft of the framework, which goes out for open consultation before a final draft is produced. Following approval by the BAPM Executive Committee, the final framework together with a detailed response to feedback received during the consultation process is published and thereafter freely available on the BAPM website. Frameworks for Practice are evidence-based whenever possible; where no evidence exists the recommendations are established by consensus. As a relatively small organisation funded almost entirely by member subscriptions, BAPM is not resourced to produce formal guidelines, but rather an expert consensus document informed by UK practice that networks could use to produce local protocols and guide-lines suitable for the needs of their own neonatal units. Our practice of publishing the full consultation allows practitioners to better under-stand the rationale behind BAPM Frameworks for Practice and ensures that they are practical and truly consensus documents.
Perinatal Management of Extreme Preterm Birth before 27 Weeks of Gestation (2019)
This framework was developed in light of evidence of improving outcomes for extremely preterm babies and evolving national and international changes in the approach to their care.
The recommendations of the 2019 framework differ from previous guidance published in 2008 in several ways. The importance of family-centred care is highlighted, helping to ensure that management of labour, birth and the immediate neonatal period reflects the wishes and values of the mother and her partner, informed and supported by consultation and in partnershipwith obstetric and neonatal professionals.
Lots of data demonstrate improved outcomes for extremely preterm babies born and cared for in tertiary level maternity and neonatal facilities and we strongly recommend that extremely preterm babies for whom, after informed consultation with parents, potentially life-sustaining care is planned should be born in maternity units co-located with a designated NICU unless in utero transfer is impractical or considered to be unsafe. This requires understanding, communication and close cooperation between maternity, obstetric and neonatal practitioners.
Another significant change in BAPM guidance is the removal of absolute gestational age cut offs for management decisions. Prognosis improves steadily with increasing gestation, reflected in current practice whereby potentially life-sustaining care is more likely to be offered for the baby towards the end of each gestational week. We recommend that an assessment of the baby’s prognosis should be made by senior members of the obstetric and neonatal team and then discussed with the parents. The framework contains lots of advice for practitioners on how to convey information to parents in a way that is easily understood, including an infographic developed with parental input (FIGURE 1). This downloadable infographic helps to explain current outcomes for extremely preterm infants, based on recent UK and international evidence.
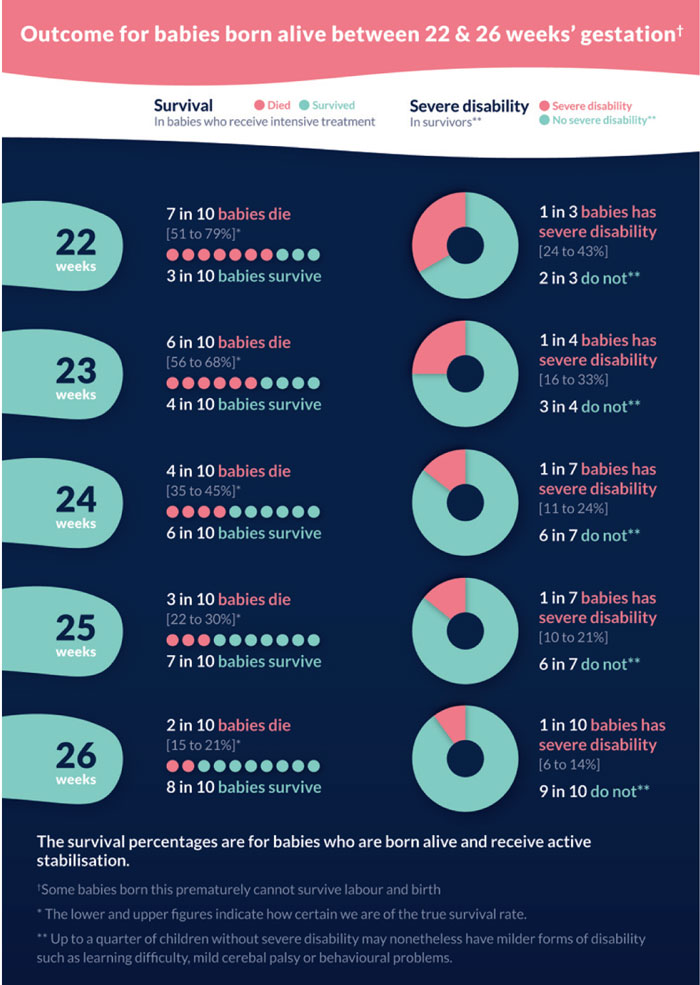
FIGURE 1 The infograph to help explain current outcomes for extremely preterm infants.
The framework guides staff through risk assessment for the baby with the aim of stratifying the risk of a poor outcome into one of three groups:
- extremely high risk (>90% chance of death or of surviving with severe disability)
- high risk (50-90% chance of death or of surviving with severe disability)
- moderate risk (<50% chance of death or of surviving with severe disability).
Factors that help to determine the risk category are gestational age, fetal growth, sex, single or multiple pregnancy, administration of antenatal steroids and place of birth.
Recognising the right of parents to choose, the framework recommends that for fetuses/babies at extremely high risk, palliative (comfort focused) care would be the usual course of management. This is most likely to apply for babies who have only just attained 22 weeks of gestation and where there are adverse factors, eg precipitate labour outside of a tertiary maternity unit. In such cases antenatal transfer, even if feasible, is unlikely to benefit the family and would generally not be appropriate. For fetuses/babies at moderate risk, active, potentially life-sustaining care would usually be planned for the baby, and obstetric management should aim to optimise the baby’s condition at birth, with in utero transfer as appropriate. For fetuses/babies at high risk of poor outcome, the decision to provide either active (survival focused) management or palliative care should be based primarily on the wishes of the parents.
In general, feedback to the consultation process was very favourable, and no one disagreed with our strong recommendation that active care should not be offered at gestations below 22+0 weeks. Several persons and organisations questioned the use of only ‘severe’ disability in addition to death in describing an unfavourable outcome; the reason for this was the ethical point of view that life or death decisions (ie whether to offer potentially life-sustaining care at birth) should be based only on outcomes that could be considered not to be in the baby’s best interests. Furthermore, for the vast majority of extremely preterm babies, neurodevelopmental disability is impossible to predict at birth. In response to feedback we did, however, modify information for parents to better describe the implications of lesser degrees of neurodisability.
The revised Framework for Practice on management of extreme preterm birth has attracted much attention across the UK, and BAPM has contributed to several network meetings on this topic. We are heartened to have heard much constructive discussion between obstetric and neonatal colleagues – the founders of the British Association of Perinatal Medicine would be truly proud!
In 2020 BAPM plans to facilitate a survey on how the revised framework has affected UK practice and we will also be working closely with the National Perinatal Epidemiology Unit and MBRRACE-UK to continue collecting quality data and to investigate whether the UK should have a common approach to stabilising the most extremely preterm babies. Watch out for this and please do contribute.
Enhancing Shared Decision Making in Neonatal Care (2019)
This framework recommends that parents should be included in making decisions about their baby’s care. The document reflects the move towards information-sharing and individualised decision-making and the role of consent within this. Since the publication of the BAPM Good Practice Framework for Consent (2004), there have been many advances in neonatal care and widely a move toward a less paternalistic model of health care with a paradigm shift in how the UK courts view standards of information disclosure and consent. In keeping with our practice of family-integrated care, it is the legal and ethical right of parents to be included in decision-making about their baby’s care.
The framework contains eight principles of shared decision-making and helps healthcare professionals walk the difficult line between fully including parents and carers in decision-making about their child and burdening the families with too much responsibility.
Calculating Unit Cot Numbers and Nurse Staffing Establishment and Determining Cot Capacity (2019)
This document provides supplementary guidance to the BAPM Framework for Practice on Service Standards for Hospitals Providing Neonatal Care (third edition, 2010) and aims to support staff in busy units to make decisions around short-term neonatal unit closure based on a variety of criteria, while always bearing in mind the best interests of families as well as neonatal unit staff.
BAPM remains fully committed to neonatal nurse-to-baby ratios of 1:1, 1:2 and 1:4 for varying levels of dependency, but we recognise that services may be stretched at times and that moving mothers and babies when optimal nurse staffing ratios cannot be met is not entirely without risk. This document was rewritten after initial consultation to make it clearer that guidance regarding optimal nurse staffing (as described in the BAPM Service Standards for Hospitals Providing Neonatal Care, 2010) should continue to be the basis for calculation of the nursing staff establishment of a neonatal unit, despite the fact that many units regularly struggle to attain these staffing levels. We hope that staff will find it helpful.
New topics
Anyone can suggest a topic for a future BAPM Framework for Practice. If there is an area of neonatal care that you think could benefit from a national framework please contact the BAPM office with your proposal. Suggestions are reviewed by the BAPM Executive Committee and, if it is agreed that a framework on the suggested topic would benefit the neonatal community, then a working group will be formed (and you may well be invited tobe on it).
BAPM’s vision is for every baby and their family in the British Isles to receive the highest standard of perinatal care. We also provide support and advocacy for perinatal professionals. If you are not already a member, please check out the BAPM website (www.bapm.org) and consider joining us today.
Or read this article in our
Tablet/iPad edition
