

Challenges in reducing central line-associated bloodstream infections in a tertiary neonatal unit: an ongoing quality improvement project
Central line-associated bloodstream infections (CLABSI) in neonates can lead to increased mortality risk, prolonged neonatal intensive care unit stays, increased costs of care and poor neurodevelopmental outcomes. The potential cause and effect relationships for CLABSI were studied by the neonatal unit at Princess Royal Maternity Glasgow to identify targets for improvement that would be likely to lead to positive change. Incremental QI-based interventions yielded a modest but sustained improvement in average CLABSI rates.
Asma Yasmeen
Consultant Neonatologist, NHS Fife (formerly Specialty Doctor, Neonatal Unit, Princess Royal Maternity Glasgow)
asmayasmeen@nhs.net
Joan McCaffer
Neonatal Nurse, Neonatal Unit, Princess Royal Maternity Glasgow (now retired)
Brian Jones
Professor and Consultant Microbiologist, Department of Microbiology, Glasgow Royal Infirmary
Chris Lilley
Consultant Neonatologist, Neonatal Unit, Princess Royal Maternity Glasgow and Training Programme Director, West of Scotland
Central line-associated bloodstream infections (CLABSI) in neonates can lead to increased mortality risk, prolonged neonatal intensive care unit stays, increased costs of care and poor neurodevelopmental outcomes.
The National Neonatal Audit Programme (NNAP) defines CLABSI as laboratory confirmed positive growth from a blood culture in a patient with a central line in place after 72 hours of birth.
CLABSI rates and quality improvement (QI)
Our tertiary neonatal unit at Princess Royal Maternity Glasgow started participating in the Scottish Patient Safety Programme (SPSP) in 2014-15.
In addition, since 2016 NNAP has utilised the BadgerNet database to benchmark data on CLABSI rates for neonatal units across the UK.
The CLABSI rate is measured as the total number of CLABSI episodes per 1,000 central line days. The CLABSI rate in the neonatal unit at Princess Royal Maternity for the first half of 2015 was 25.5 per 1,000 central line days. The CLABSI rate due to Staphylococcus aureus in 2015 was 5.6 per 1,000 central line days.
The cause and effect relationships (FIGURE 1) were studied by the unit’s infection control team to identify targets for improvement that would be likely to lead to positive change (FIGURE 2). The following were identified as leading concerns:
- contamination of blood culture samples especially after the changeover of medical staff
- poor aseptic technique during central line insertion
- poor hub care.
Data were collected from case notes, local records of compliance bundles, online patient record databases and monthly microbiology updates on bacteriology samples.
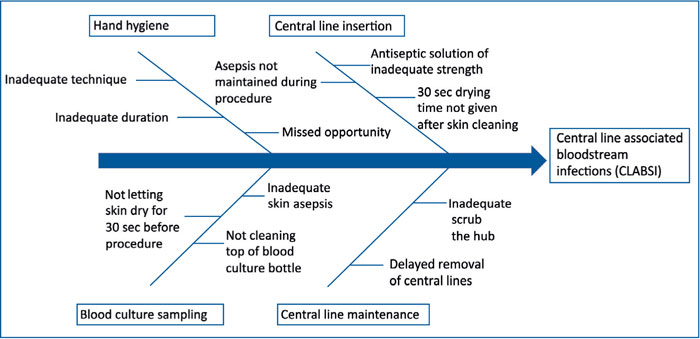
FIGURE 1 Potential cause and effect relationships for CLABSI.
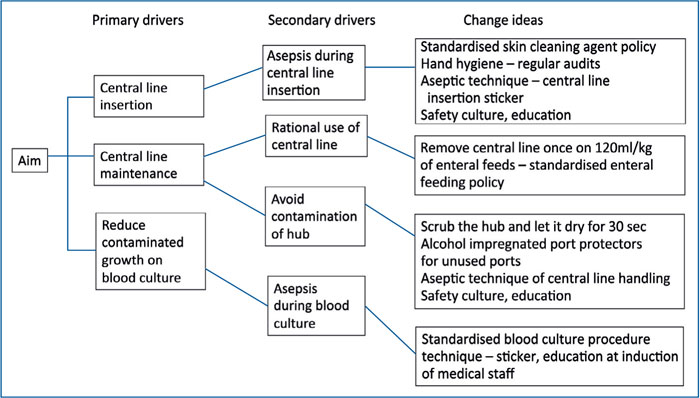
FIGURE 2 Drivers of change for reduction in CLABSI rates.
PDSA cycle 2015-16
The aim was to reduce line-related sepsis rates in accordance with SPSP to <10 per 1,000 central line days. The following changes were implemented in a step-wise manner by a series of plan-do-study-act (PDSA) cycles:
- a blood culture sticker pasted into the case notes to act as a record and prompt for proper technique
- training of medical staff during induction in the correct method of sampling for blood culture
- revision of skin disinfection solutions (gestation-specific use of either aqueous chlorhexidine (0.5%) or 70% isopropyl alcohol with chlorhexidine 2%)
- commencement of a care bundle for central line insertion and maintenance
- assembly of an infection control group.
Outcomes
CLABSI rates reduced to 22.7 per 1,000 central line days in the latter half of 2015 and 15.8 per 1,000 central line days in 2016.
PDSA cycle 2017-18
The changes planned for the next PDSA cycle were to ensure:
- alcohol impregnated port protectors for unused ports
- ‘scrubbing the hub’ and waiting for 30 seconds before re-attaching infusions
- increased training on general infection control measures
- revision of central line insertion stickers to prompt for a pause to allow skin to dry after cleaning with antiseptic solution
- further improvement in blood culture technique by the use of a timer to ensure adequate drying of antiseptic solution.
Outcomes
CLABSI rates increased in 2017 to 18.8 per 1,000 central line days, and then reduced to 11.3 per 1,000 central line days in 2018. The rise noted in 2017 points to an ongoing need for education and compliance with the changes implemented during the QI programme. Following the introduction of alcohol impregnated port protectors in July 2016, no episodes of Staphylococcus aureus CLABSI were recorded.
Conclusion
Incremental QI-based interventions have shown a modest but sustained improve-ment in our average CLABSI rates (FIGURE 3). Further work on compliance with policies, education and staff motivation, especially at induction, are required to achieve further improvement and consistent results.
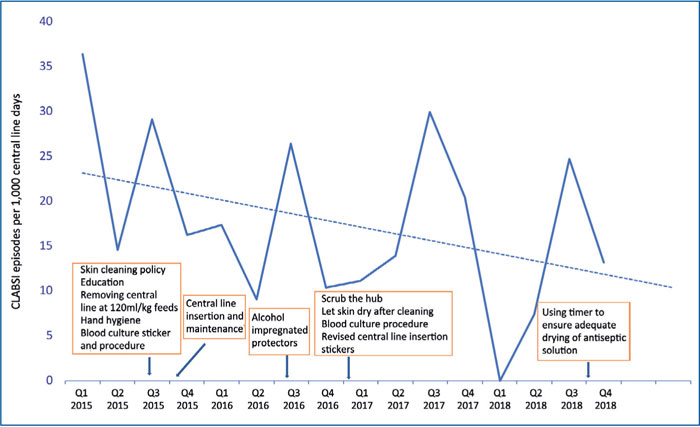
FIGURE 3 A cumulative chart of CLABSI rates (quarterly values) with trend-line, 2015-18.
This article is based on a poster presented at the REaSoN conference in 2019, which won the prize for Best Poster – Quality Improvement.
Or read this article in our
Tablet/iPad edition
